Das könnte Ihnen auch gefallen
- Casa Er 2014Dokument10 SeitenCasa Er 2014Siti HajarNoch keine Bewertungen
- Malnutrition Diagnoses in Hospitalized Patients: United States, 2010Dokument10 SeitenMalnutrition Diagnoses in Hospitalized Patients: United States, 2010MichealNoch keine Bewertungen
- Evans 2015Dokument7 SeitenEvans 2015Dr. Jaydeep MalakarNoch keine Bewertungen
- Research Agenda For Medical Cannabis in Palliative CareDokument3 SeitenResearch Agenda For Medical Cannabis in Palliative CarejclamasNoch keine Bewertungen
- Jco 2004 02 166Dokument4 SeitenJco 2004 02 166Cecilia ArgañarazNoch keine Bewertungen
- Jamainternal Heger 2023 PP 230001 1681398072.43626Dokument2 SeitenJamainternal Heger 2023 PP 230001 1681398072.43626Paola Cristini Gama SilvaNoch keine Bewertungen
- Postsepsis MorbidityDokument1 SeitePostsepsis MorbidityDaniel Enrique RubioNoch keine Bewertungen
- Hemoderivados en Cuidado CríticoDokument6 SeitenHemoderivados en Cuidado CríticoIvan Mauricio Palma BarraganNoch keine Bewertungen
- SUPER - Recom - Vaccin-ESRD-AJKD-2019Dokument9 SeitenSUPER - Recom - Vaccin-ESRD-AJKD-2019Ioana PanculescuNoch keine Bewertungen
- Improving End of Life CareDokument9 SeitenImproving End of Life CareM_LXNoch keine Bewertungen
- Improving Care For Overweight and Obese PatientsDokument5 SeitenImproving Care For Overweight and Obese PatientsJoshua DiaoNoch keine Bewertungen
- The Importance of Diagnosing and Managing ICU DeliriumDokument13 SeitenThe Importance of Diagnosing and Managing ICU DeliriumPablo RamirezNoch keine Bewertungen
- 1 - Educación Nutricional en La Escuela de MedicinaDokument2 Seiten1 - Educación Nutricional en La Escuela de MedicinakbuhringNoch keine Bewertungen
- JA A D: Saabg@health - Missouri.eduDokument3 SeitenJA A D: Saabg@health - Missouri.eduValentina AdindaNoch keine Bewertungen
- The AIDS Fighters - Brighthope, Ian Fitzgerald, PeterDokument196 SeitenThe AIDS Fighters - Brighthope, Ian Fitzgerald, Peterpdf ebook free download100% (1)
- Managing a Patient With Recurrent Gout AttacksDokument10 SeitenManaging a Patient With Recurrent Gout AttacksJesús Evangelista GomerNoch keine Bewertungen
- What'S The: Verdict?Dokument3 SeitenWhat'S The: Verdict?Cathy GabroninoNoch keine Bewertungen
- Protein and Calorie Requirements Associated With The Presence of ObesityDokument8 SeitenProtein and Calorie Requirements Associated With The Presence of ObesityRaman ChaudharyNoch keine Bewertungen
- 336.nut in Clin Prac - 2017 - Dickerson - Protein and Calorie Requirements Associated With The Presence of ObesityDokument8 Seiten336.nut in Clin Prac - 2017 - Dickerson - Protein and Calorie Requirements Associated With The Presence of ObesitytereNoch keine Bewertungen
- Journal: in This IssueDokument20 SeitenJournal: in This IssueLaura ZahariaNoch keine Bewertungen
- Kleinsinge 2018 - No AdherenciaDokument3 SeitenKleinsinge 2018 - No AdherenciaJuan camiloNoch keine Bewertungen
- Kleinsinge 2018 - No AdherenciaDokument3 SeitenKleinsinge 2018 - No AdherenciaJuan camiloNoch keine Bewertungen
- Precision Obesity Care On The Horizon: CirculationDokument3 SeitenPrecision Obesity Care On The Horizon: CirculationCarlosMoscosoNoch keine Bewertungen
- 1 s2.0 S2405457720301169 MainDokument16 Seiten1 s2.0 S2405457720301169 MainjvracuyaNoch keine Bewertungen
- 727 Outcomes of Antibiotic Use in Ischemic ColitisDokument2 Seiten727 Outcomes of Antibiotic Use in Ischemic ColitisDonNoch keine Bewertungen
- WischmeyerSurgNutritPOET20 tcm1423-138070Dokument12 SeitenWischmeyerSurgNutritPOET20 tcm1423-138070ckg5r6ykncNoch keine Bewertungen
- Harrisons Principles of Internal Medicine 21st Edition Vol 1 Vol Split PDF 1694700703964Dokument73 SeitenHarrisons Principles of Internal Medicine 21st Edition Vol 1 Vol Split PDF 1694700703964Clorinda RodriguezNoch keine Bewertungen
- Hospitalistas y Medicos de Familia, EditorialDokument1 SeiteHospitalistas y Medicos de Familia, EditorialJuan pablo Lopez MuñosNoch keine Bewertungen
- Jamainternal Gupta 2024 Oi 240004 1710785795.21061Dokument9 SeitenJamainternal Gupta 2024 Oi 240004 1710785795.21061Jose Artur AlbuquerqueNoch keine Bewertungen
- Williams 2020, Tutorial Devolopment and Implementation of A Multidisciplinary Preoperative Nutrition Optimization ClinicDokument12 SeitenWilliams 2020, Tutorial Devolopment and Implementation of A Multidisciplinary Preoperative Nutrition Optimization Clinicdiana perezNoch keine Bewertungen
- J Parenter Enteral Nutr - 2021 - Compher - Guidelines For The Provision of Nutrition Support Therapy in The AdultDokument30 SeitenJ Parenter Enteral Nutr - 2021 - Compher - Guidelines For The Provision of Nutrition Support Therapy in The AdultPabloNoch keine Bewertungen
- Nutrition Status and Risk Factors Associated With Length of Hospital Stay For Surgical PatientsDokument8 SeitenNutrition Status and Risk Factors Associated With Length of Hospital Stay For Surgical PatientsFarida MufidatiNoch keine Bewertungen
- ASPEN - Suplemental Parenteral Nutrition - Review of The Literature and Current Nutriton GuidelinesDokument11 SeitenASPEN - Suplemental Parenteral Nutrition - Review of The Literature and Current Nutriton GuidelinesRoberto Cárdenas GarcíaNoch keine Bewertungen
- J Parenter Enteral Nutr - 2021 - Compher - Guidelines For The Provision of Nutrition Support Therapy in The AdultDokument30 SeitenJ Parenter Enteral Nutr - 2021 - Compher - Guidelines For The Provision of Nutrition Support Therapy in The Adultsulemi castañonNoch keine Bewertungen
- International Journal of Gerontology: Thiago J. Avelino-Silva, Omar JaluulDokument6 SeitenInternational Journal of Gerontology: Thiago J. Avelino-Silva, Omar JaluulKaye Antonette AntioquiaNoch keine Bewertungen
- LRDokument22 SeitenLRمالك مناصرةNoch keine Bewertungen
- Obesity ManagentDokument54 SeitenObesity ManagentHugo David CoronelNoch keine Bewertungen
- Aspen Guidelines SurgicalDokument10 SeitenAspen Guidelines SurgicalJeshuanna DelgadoNoch keine Bewertungen
- Author Reply: BJU Int 2011 108 (Suppl 2)Dokument1 SeiteAuthor Reply: BJU Int 2011 108 (Suppl 2)Selliana Maretha Wijaya KusumaNoch keine Bewertungen
- NEJM Journal Watch Year in Review 2021Dokument20 SeitenNEJM Journal Watch Year in Review 2021Jaime DehaisNoch keine Bewertungen
- Acute Renal FailureDokument54 SeitenAcute Renal FailureNiala Almario100% (1)
- 1252-Article Text-5341-2-10-20200212Dokument6 Seiten1252-Article Text-5341-2-10-20200212Lizette AntonioNoch keine Bewertungen
- Competencies in Palliative Care For Cardiology FellowsDokument4 SeitenCompetencies in Palliative Care For Cardiology Fellowsandrey prawiroNoch keine Bewertungen
- Addressing Medicine's Bias Against Patients Who Are OverweightDokument3 SeitenAddressing Medicine's Bias Against Patients Who Are OverweightSean ChoNoch keine Bewertungen
- ARM en ICDokument11 SeitenARM en ICxLarcXDNoch keine Bewertungen
- 2011 Corrigan - Nutrition in Stroke PatientsDokument11 Seiten2011 Corrigan - Nutrition in Stroke PatientsAmy100% (1)
- Commentary: Nutritional Assessment and Length of Hospital StayDokument2 SeitenCommentary: Nutritional Assessment and Length of Hospital StayNjeodoNoch keine Bewertungen
- Medical Nutrition Therapy in Chronic Renal Disease: A Case StudyDokument6 SeitenMedical Nutrition Therapy in Chronic Renal Disease: A Case StudysarahNoch keine Bewertungen
- clinical nursing judgementDokument5 Seitenclinical nursing judgementapi-740444719Noch keine Bewertungen
- Carroll2017 PDFDokument1 SeiteCarroll2017 PDFLuisNoch keine Bewertungen
- Advantages of EnteralDokument11 SeitenAdvantages of EnteralClarestaNoch keine Bewertungen
- Vitamin C Deficiency in A University Teaching2008Dokument7 SeitenVitamin C Deficiency in A University Teaching2008Rossmery Mirella Vera PadillaNoch keine Bewertungen
- Geriatric Preoperative Optimization: A ReviewDokument10 SeitenGeriatric Preoperative Optimization: A Reviewalejandro montesNoch keine Bewertungen
- 2nd PeritonitisDokument11 Seiten2nd PeritonitisqweqweqwNoch keine Bewertungen
- Nutritional Assessment of The Critically Ill PatientDokument8 SeitenNutritional Assessment of The Critically Ill PatientDevani Bagus Aprinda0% (1)
- Stage III-B Cervical-Cancer of Young Age in Medical, Bioethics and Clinical Ethics PerspectivesDokument6 SeitenStage III-B Cervical-Cancer of Young Age in Medical, Bioethics and Clinical Ethics PerspectivesmusdalifahNoch keine Bewertungen
- s13054 017 1690 5Dokument16 Seitens13054 017 1690 5Anonymous SvlxqQeiNoch keine Bewertungen
- 2007 Pharmacy Times Inpatientglucosecontrol Szumita Greenwood Anger PendergrassDokument12 Seiten2007 Pharmacy Times Inpatientglucosecontrol Szumita Greenwood Anger Pendergrassnia rahayu wNoch keine Bewertungen
- Antibiotic Prophylaxis For Infective Endocarditis: CirculationDokument3 SeitenAntibiotic Prophylaxis For Infective Endocarditis: Circulationjagjit singhNoch keine Bewertungen
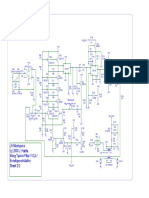
- JH Minotaurus Schematic p2 - Moog Taurus Filter VCA ENV EmulatorDokument1 SeiteJH Minotaurus Schematic p2 - Moog Taurus Filter VCA ENV EmulatorcrackintheshatNoch keine Bewertungen
- JH Minotaurus Schematic p1 - Moog Taurus Filter VCA ENV EmulatorDokument1 SeiteJH Minotaurus Schematic p1 - Moog Taurus Filter VCA ENV EmulatorcrackintheshatNoch keine Bewertungen
- Eviews F HerapeuticsDokument17 SeitenEviews F HerapeuticscrackintheshatNoch keine Bewertungen
- LVL - LOK-500 v1.13 SWITCH WIRINGDokument1 SeiteLVL - LOK-500 v1.13 SWITCH WIRINGcrackintheshatNoch keine Bewertungen
- Moog MF-101 LPF SchematicsDokument5 SeitenMoog MF-101 LPF SchematicscrackintheshatNoch keine Bewertungen
- Buddha CompDokument1 SeiteBuddha CompcrackintheshatNoch keine Bewertungen
- Match Transistors for Circuits with <40mΩ MismatchDokument5 SeitenMatch Transistors for Circuits with <40mΩ MismatchcrackintheshatNoch keine Bewertungen
- MF 101Dokument14 SeitenMF 101Kara JohnstonNoch keine Bewertungen
- Analysis of the SMR-4 VCF/VCA BoardDokument10 SeitenAnalysis of the SMR-4 VCF/VCA BoardcrackintheshatNoch keine Bewertungen
- Ladder Filter Design, Fabrication, & Measurement - EECS 142 Lab 3 Background ReadingDokument27 SeitenLadder Filter Design, Fabrication, & Measurement - EECS 142 Lab 3 Background ReadingcrackintheshatNoch keine Bewertungen
- LVL - Lok-500 v1.13 SchematicDokument1 SeiteLVL - Lok-500 v1.13 SchematiccrackintheshatNoch keine Bewertungen
- Russian FET CompressorDokument15 SeitenRussian FET CompressorcrackintheshatNoch keine Bewertungen
- LVL - LOK-500 v1.13 BOMDokument1 SeiteLVL - LOK-500 v1.13 BOMcrackintheshatNoch keine Bewertungen
- EHX Black Finger PDFDokument1 SeiteEHX Black Finger PDFГеоргий Ельцов100% (1)
- Electronics Today Magazine - January 1985 (ETI)Dokument76 SeitenElectronics Today Magazine - January 1985 (ETI)crackintheshat100% (1)
- Basic Transformer Hook Up DataDokument2 SeitenBasic Transformer Hook Up DatacrackintheshatNoch keine Bewertungen
- Pirani Gauge JST - 20131220Dokument9 SeitenPirani Gauge JST - 20131220crackintheshatNoch keine Bewertungen
- EC445 Final - Paper1Dokument22 SeitenEC445 Final - Paper1crackintheshatNoch keine Bewertungen
- EnigmaDokument2 SeitenEnigmaDwight JonesNoch keine Bewertungen
- Outcome of A Histamine-Restricted Diet Based On Chart Audit - JANICE M. VICKERSTAFF JONEJA PHD RDNDokument15 SeitenOutcome of A Histamine-Restricted Diet Based On Chart Audit - JANICE M. VICKERSTAFF JONEJA PHD RDNcrackintheshatNoch keine Bewertungen
- Summary of Terrorist Attacks of September 11, 2001Dokument6 SeitenSummary of Terrorist Attacks of September 11, 2001ShaktikumarNoch keine Bewertungen
- Barriga de Trigo - William DavisDokument19 SeitenBarriga de Trigo - William Davisfilipecosta1993Noch keine Bewertungen
- Amplifier Classification and Op-Amp ECG ApplicationDokument60 SeitenAmplifier Classification and Op-Amp ECG ApplicationcrackintheshatNoch keine Bewertungen
- Histamine and Histamine Intolerance1 3 Laura Maintz and Natalija Novak Znu00507001185 PDFDokument12 SeitenHistamine and Histamine Intolerance1 3 Laura Maintz and Natalija Novak Znu00507001185 PDFcrackintheshatNoch keine Bewertungen
- MIT Op-Amp Lab ReportDokument20 SeitenMIT Op-Amp Lab ReportcrackintheshatNoch keine Bewertungen
- Lab 06 - Mosfet & JfetsDokument64 SeitenLab 06 - Mosfet & JfetscrackintheshatNoch keine Bewertungen
- GP6 Users Manual enDokument61 SeitenGP6 Users Manual enJosé Antonio TapiaNoch keine Bewertungen
- Lab 2 - Transistor BiasDokument12 SeitenLab 2 - Transistor Biascrackintheshat100% (1)
- Lab 07 - Op-AmpsDokument49 SeitenLab 07 - Op-AmpscrackintheshatNoch keine Bewertungen
- Lab 05 - 3 Stage AmpliferDokument47 SeitenLab 05 - 3 Stage AmplifercrackintheshatNoch keine Bewertungen
- Diagnostic Diabetes: Diagnosing Maturity-Onset Diabetes of The Young (MODY)Dokument32 SeitenDiagnostic Diabetes: Diagnosing Maturity-Onset Diabetes of The Young (MODY)Christian SalimNoch keine Bewertungen
- Erectile Dysfunction Cure - How To Cure ED Naturally & Quickly & Enjoy Your Intimate Life (Jelqing, Male Enhancement, ED Cure, Erectile Dysfunction, Infertility) PDFDokument97 SeitenErectile Dysfunction Cure - How To Cure ED Naturally & Quickly & Enjoy Your Intimate Life (Jelqing, Male Enhancement, ED Cure, Erectile Dysfunction, Infertility) PDFWaleedNoch keine Bewertungen
- Diabetes and Gum Disease: Does Oral Health Matter?: Imogen Midwood, Penny HodgeDokument4 SeitenDiabetes and Gum Disease: Does Oral Health Matter?: Imogen Midwood, Penny HodgeNovena DpNoch keine Bewertungen
- International Nursing Conference Abstracts - AINEC 2018Dokument42 SeitenInternational Nursing Conference Abstracts - AINEC 2018Rika Fatmadona100% (1)
- Diabetic Retinopathy by-DuaneBryantMDDokument7 SeitenDiabetic Retinopathy by-DuaneBryantMDduanebryantmdNoch keine Bewertungen
- Social Orientation and Diabetes Distress in Japanese and American PatientsDokument7 SeitenSocial Orientation and Diabetes Distress in Japanese and American PatientsDebby Syahru RomadlonNoch keine Bewertungen
- Raymond Lo - The Year of The RatDokument4 SeitenRaymond Lo - The Year of The Ratay2004janNoch keine Bewertungen
- Ispad 2014Dokument290 SeitenIspad 2014Sheyla Alegre Pariona100% (1)
- Funda (Course Audit)Dokument16 SeitenFunda (Course Audit)Kath-Kath Cubillan RanayNoch keine Bewertungen
- Animal Aloksan PDFDokument14 SeitenAnimal Aloksan PDFTrias Ilmi PramudikaNoch keine Bewertungen
- Evaluation of Protective Effects of Euphorbia thymifolia Linn against Streptozotocin induced Diabetic Neuropathy in RatsDokument12 SeitenEvaluation of Protective Effects of Euphorbia thymifolia Linn against Streptozotocin induced Diabetic Neuropathy in Ratsrr48843Noch keine Bewertungen
- Basal Bolus InsulinDMT22009Dokument92 SeitenBasal Bolus InsulinDMT22009scribdNoch keine Bewertungen
- Current Challenges in Non-Invasive Insulin Delivery Systems A Comparative ReviewDokument26 SeitenCurrent Challenges in Non-Invasive Insulin Delivery Systems A Comparative Reviewridley45Noch keine Bewertungen
- FructosuriaDokument2 SeitenFructosuriaKaranja GitauNoch keine Bewertungen
- UntitledDokument54 SeitenUntitledapi-198310771Noch keine Bewertungen
- Non Communicable DiseasesDokument13 SeitenNon Communicable Diseaseszzzsubedi100% (1)
- GlimepirideDokument12 SeitenGlimepirideMobahil AhmadNoch keine Bewertungen
- Shoulder DystociaDokument13 SeitenShoulder Dystociarolla_hiraNoch keine Bewertungen
- 07 NovDokument32 Seiten07 NovEditorial TeamNoch keine Bewertungen
- Laboratory Tests To Evaluate Fluid StatusDokument52 SeitenLaboratory Tests To Evaluate Fluid StatusLester Exconde Alfonso0% (1)
- AMC MCQ Exam 2 Questions & Answer KeyDokument38 SeitenAMC MCQ Exam 2 Questions & Answer KeyVasile Rusnac100% (4)
- The Social Psychology of Exercise and Sport 2005 (For LydiaDokument280 SeitenThe Social Psychology of Exercise and Sport 2005 (For LydiaStephen Ladiator Cooper Shirley100% (1)
- Natural Medicines Used in The Traditional Chinese Medical System For Therapy of Diabetes MellitusDokument21 SeitenNatural Medicines Used in The Traditional Chinese Medical System For Therapy of Diabetes MellitusparibashaiNoch keine Bewertungen
- David Perlmutter Focus Autoimmune PDFDokument23 SeitenDavid Perlmutter Focus Autoimmune PDFutpal_thakar100% (6)
- Anatomia SufletuluiDokument1 SeiteAnatomia SufletuluiAlexandrina DeaşNoch keine Bewertungen
- Other Health Impairment Fact SheetDokument8 SeitenOther Health Impairment Fact SheetNational Dissemination Center for Children with DisabilitiesNoch keine Bewertungen
- Dka and HonkDokument30 SeitenDka and HonkignasachyntiaNoch keine Bewertungen
- Nutrition ManualDokument405 SeitenNutrition ManualRaghavendra Prasad100% (1)
- Management of Diabetes: DR Rukman Mecca M I 51 ST Batch Calicut Med CollegeDokument47 SeitenManagement of Diabetes: DR Rukman Mecca M I 51 ST Batch Calicut Med CollegeRukman MeccaNoch keine Bewertungen
- DietandCVDriskfactorsinBotswana Kwape PhDthesis2012 (1) (001-025)Dokument25 SeitenDietandCVDriskfactorsinBotswana Kwape PhDthesis2012 (1) (001-025)Indri Reskiawanti GalibNoch keine Bewertungen
- The Obesity Code: Unlocking the Secrets of Weight LossVon EverandThe Obesity Code: Unlocking the Secrets of Weight LossBewertung: 5 von 5 Sternen5/5 (4)
- The Diabetes Code: Prevent and Reverse Type 2 Diabetes NaturallyVon EverandThe Diabetes Code: Prevent and Reverse Type 2 Diabetes NaturallyBewertung: 5 von 5 Sternen5/5 (1)
- The Arm: Inside the Billion-Dollar Mystery of the Most Valuable Commodity in SportsVon EverandThe Arm: Inside the Billion-Dollar Mystery of the Most Valuable Commodity in SportsBewertung: 4 von 5 Sternen4/5 (49)
- Proteinaholic: How Our Obsession with Meat Is Killing Us and What We Can Do About ItVon EverandProteinaholic: How Our Obsession with Meat Is Killing Us and What We Can Do About ItBewertung: 4.5 von 5 Sternen4.5/5 (19)
- The Fast800 Diet: Discover the Ideal Fasting Formula to Shed Pounds, Fight Disease, and Boost Your Overall HealthVon EverandThe Fast800 Diet: Discover the Ideal Fasting Formula to Shed Pounds, Fight Disease, and Boost Your Overall HealthBewertung: 5 von 5 Sternen5/5 (37)
- The Candida Cure: The 90-Day Program to Balance Your Gut, Beat Candida, and Restore Vibrant HealthVon EverandThe Candida Cure: The 90-Day Program to Balance Your Gut, Beat Candida, and Restore Vibrant HealthNoch keine Bewertungen
- Summary: Fast Like a Girl: A Woman’s Guide to Using the Healing Power of Fasting to Burn Fat, Boost Energy, and Balance Hormones: Key Takeaways, Summary and AnalysisVon EverandSummary: Fast Like a Girl: A Woman’s Guide to Using the Healing Power of Fasting to Burn Fat, Boost Energy, and Balance Hormones: Key Takeaways, Summary and AnalysisBewertung: 3 von 5 Sternen3/5 (2)
- Forever Strong: A New, Science-Based Strategy for Aging WellVon EverandForever Strong: A New, Science-Based Strategy for Aging WellNoch keine Bewertungen
- Allen Carr's Easy Way for Women to Lose Weight: The original Easyway methodVon EverandAllen Carr's Easy Way for Women to Lose Weight: The original Easyway methodBewertung: 4.5 von 5 Sternen4.5/5 (18)
- Metabolism Revolution: Lose 14 Pounds in 14 Days and Keep It Off for LifeVon EverandMetabolism Revolution: Lose 14 Pounds in 14 Days and Keep It Off for LifeNoch keine Bewertungen
- Glucose Goddess Method: A 4-Week Guide to Cutting Cravings, Getting Your Energy Back, and Feeling AmazingVon EverandGlucose Goddess Method: A 4-Week Guide to Cutting Cravings, Getting Your Energy Back, and Feeling AmazingBewertung: 5 von 5 Sternen5/5 (59)
- Eat to Lose, Eat to Win: Your Grab-n-Go Action Plan for a Slimmer, Healthier YouVon EverandEat to Lose, Eat to Win: Your Grab-n-Go Action Plan for a Slimmer, Healthier YouNoch keine Bewertungen
- Happy Gut: The Cleansing Program to Help You Lose Weight, Gain Energy, and Eliminate PainVon EverandHappy Gut: The Cleansing Program to Help You Lose Weight, Gain Energy, and Eliminate PainBewertung: 3.5 von 5 Sternen3.5/5 (6)
- Grit & Grace: Train the Mind, Train the Body, Own Your LifeVon EverandGrit & Grace: Train the Mind, Train the Body, Own Your LifeBewertung: 4 von 5 Sternen4/5 (3)
- How to Be Well: The 6 Keys to a Happy and Healthy LifeVon EverandHow to Be Well: The 6 Keys to a Happy and Healthy LifeBewertung: 5 von 5 Sternen5/5 (1)
- Summary of Mary Claire Haver's The Galveston DietVon EverandSummary of Mary Claire Haver's The Galveston DietBewertung: 5 von 5 Sternen5/5 (1)
- Keto Friendly Recipes: Easy Keto For Busy PeopleVon EverandKeto Friendly Recipes: Easy Keto For Busy PeopleBewertung: 2 von 5 Sternen2/5 (1)
- Power Souping: 3-Day Detox, 3-Week Weight-Loss PlanVon EverandPower Souping: 3-Day Detox, 3-Week Weight-Loss PlanBewertung: 3.5 von 5 Sternen3.5/5 (3)
- The Longevity Plan: Seven Life-Transforming Lessons from Ancient ChinaVon EverandThe Longevity Plan: Seven Life-Transforming Lessons from Ancient ChinaNoch keine Bewertungen
- The Raw Food Detox Diet: The Five-Step Plan for Vibrant Health and Maximum Weight LossVon EverandThe Raw Food Detox Diet: The Five-Step Plan for Vibrant Health and Maximum Weight LossBewertung: 4 von 5 Sternen4/5 (22)
- The Toxin Solution: How Hidden Poisons in the Air, Water, Food, and Products We Use Are Destroying Our Health—AND WHAT WE CAN DO TO FIX ITVon EverandThe Toxin Solution: How Hidden Poisons in the Air, Water, Food, and Products We Use Are Destroying Our Health—AND WHAT WE CAN DO TO FIX ITBewertung: 5 von 5 Sternen5/5 (1)
- Lose Weight by Eating: 130 Amazing Clean-Eating Makeovers for Guilt-Free Comfort FoodVon EverandLose Weight by Eating: 130 Amazing Clean-Eating Makeovers for Guilt-Free Comfort FoodBewertung: 2 von 5 Sternen2/5 (1)
- Rapid Weight Loss Hypnosis: How to Lose Weight with Self-Hypnosis, Positive Affirmations, Guided Meditations, and Hypnotherapy to Stop Emotional Eating, Food Addiction, Binge Eating and MoreVon EverandRapid Weight Loss Hypnosis: How to Lose Weight with Self-Hypnosis, Positive Affirmations, Guided Meditations, and Hypnotherapy to Stop Emotional Eating, Food Addiction, Binge Eating and MoreBewertung: 5 von 5 Sternen5/5 (17)
- Ultrametabolism: The Simple Plan for Automatic Weight LossVon EverandUltrametabolism: The Simple Plan for Automatic Weight LossBewertung: 4.5 von 5 Sternen4.5/5 (28)
- Think Yourself Thin: A 30-Day Guide to Permanent Weight LossVon EverandThink Yourself Thin: A 30-Day Guide to Permanent Weight LossBewertung: 4.5 von 5 Sternen4.5/5 (22)
- The Ultimate Volumetrics Diet: Smart, Simple, Science-Based Strategies for Losing Weight and Keeping It OffVon EverandThe Ultimate Volumetrics Diet: Smart, Simple, Science-Based Strategies for Losing Weight and Keeping It OffNoch keine Bewertungen