Das könnte Ihnen auch gefallen
- Guide +++++ PDFDokument110 SeitenGuide +++++ PDFimtiyazh8567% (3)
- A To Z Orthodontics MCQDokument112 SeitenA To Z Orthodontics MCQUjjwal Pyakurel100% (4)
- A To Z Orthodontics Vol 25 Orthodontic MCQDokument113 SeitenA To Z Orthodontics Vol 25 Orthodontic MCQelie33% (3)
- Atoz Orthodontics: Rthodontic MCQDokument112 SeitenAtoz Orthodontics: Rthodontic MCQAbdo SerboutiNoch keine Bewertungen
- Class I and Class II MalocclusionDokument13 SeitenClass I and Class II MalocclusionmelNoch keine Bewertungen
- Classification of MalocclusionDokument51 SeitenClassification of MalocclusionYuvashreeNoch keine Bewertungen
- Class 2 Div 1 MyDokument146 SeitenClass 2 Div 1 Mysonal agarwal50% (2)
- Classification of Malocclusion Project MGM DentalDokument62 SeitenClassification of Malocclusion Project MGM Dentaljoysanaria827390% (10)
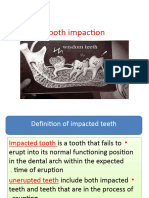
- Impacted Teeth GuideDokument125 SeitenImpacted Teeth Guideshagun singh0% (1)
- Ortho DTPDokument11 SeitenOrtho DTPFathima ShaminNoch keine Bewertungen
- Classifications of OcclusionDokument2 SeitenClassifications of Occlusionkbkim7Noch keine Bewertungen
- Figure 11a.: Class II, Division 1 Occurs When The Permanent First Molars Are in Class II and The Permanent MaxillaryDokument2 SeitenFigure 11a.: Class II, Division 1 Occurs When The Permanent First Molars Are in Class II and The Permanent MaxillaryniveditakartikNoch keine Bewertungen
- Understanding Malocclusion ClassificationDokument15 SeitenUnderstanding Malocclusion ClassificationBlack Hack HakerNoch keine Bewertungen
- Ceramah 2Dokument25 SeitenCeramah 2Davinna SatgunarajahNoch keine Bewertungen
- 1 - Introduction in OrthodonticsDokument4 Seiten1 - Introduction in OrthodonticsZakria Al-HadadNoch keine Bewertungen
- The Business of DentistryDokument4 SeitenThe Business of DentistryEvelyn RojsNoch keine Bewertungen
- A To Z Orthodontics. Volume 16: Class III Malocclusion: January 2013Dokument21 SeitenA To Z Orthodontics. Volume 16: Class III Malocclusion: January 2013Mohammad SaadNoch keine Bewertungen
- Molar Uprighting / Orthodontic Courses by Indian Dental AcademyDokument142 SeitenMolar Uprighting / Orthodontic Courses by Indian Dental Academyindian dental academy100% (1)
- OrthodonticDokument58 SeitenOrthodonticpawi18Noch keine Bewertungen
- Extraction in Orthodontic TreatmentDokument50 SeitenExtraction in Orthodontic Treatment2w48wt7d5bNoch keine Bewertungen
- CANINE Impaction Oral SurgeryDokument46 SeitenCANINE Impaction Oral SurgeryFourthMolar.com100% (5)
- Assignment OrthoDokument5 SeitenAssignment OrthoIgnasNoch keine Bewertungen
- Molar Distalization in Begg Technique / Orthodontic Courses by Indian Dental AcademyDokument46 SeitenMolar Distalization in Begg Technique / Orthodontic Courses by Indian Dental Academyindian dental academyNoch keine Bewertungen
- Orthodontic CaseDokument17 SeitenOrthodontic Casealexandra reginaNoch keine Bewertungen
- DR - Fidaa Impaction-1Dokument59 SeitenDR - Fidaa Impaction-1Sondos MoustafaNoch keine Bewertungen
- Management of Class Ii Division 1 MalocclusionDokument67 SeitenManagement of Class Ii Division 1 MalocclusionMahima Gupta100% (2)
- Management of Impacted TeethDokument153 SeitenManagement of Impacted Teethdr_nilofervevai2360100% (2)
- Class 2 Write UpDokument31 SeitenClass 2 Write UpPZNoch keine Bewertungen
- Orthodontics - 9th LectureDokument7 SeitenOrthodontics - 9th LectureMarwan Qasim GhNoch keine Bewertungen
- Classification of MalocclusionDokument69 SeitenClassification of MalocclusionBatman 02053Noch keine Bewertungen
- Classification of malocclusions and dental relationshipsDokument7 SeitenClassification of malocclusions and dental relationshipsWeiliem AbubakarNoch keine Bewertungen
- Methods of Space Gaining in OrthodonticsDokument41 SeitenMethods of Space Gaining in OrthodonticsAwas AwasNoch keine Bewertungen
- Abhijith B Final Year Part 1 Roll No:1Dokument24 SeitenAbhijith B Final Year Part 1 Roll No:1nath yshakNoch keine Bewertungen
- Cross Bite: by Assist. Prof. Dr. Hadi M IsmailDokument38 SeitenCross Bite: by Assist. Prof. Dr. Hadi M Ismailyounisismail935Noch keine Bewertungen
- Class IDokument56 SeitenClass IatikaNoch keine Bewertungen
- Congenitally Missing LateralDokument26 SeitenCongenitally Missing LateralAya ElsayedNoch keine Bewertungen
- CONCEPT OF NORMAL OCCLUSIONDokument39 SeitenCONCEPT OF NORMAL OCCLUSIONAlok Avinash100% (1)
- Seminar Molar DistalizationDokument130 SeitenSeminar Molar DistalizationMuhsina EyyanathilNoch keine Bewertungen
- Fixed Functional Appliances for Treatment of Class II MalocclusionsDokument35 SeitenFixed Functional Appliances for Treatment of Class II MalocclusionsAya ElsayedNoch keine Bewertungen
- Class 2 in Growing PtsDokument8 SeitenClass 2 in Growing PtsDevender KumarNoch keine Bewertungen
- CL 1 Malocclusion 5TH DR Mouayad 20200531084732Dokument57 SeitenCL 1 Malocclusion 5TH DR Mouayad 20200531084732israa fuadNoch keine Bewertungen
- Management of Impacted TeethDokument153 SeitenManagement of Impacted TeethToma Irina100% (1)
- Impacted TeethDokument69 SeitenImpacted TeethAntony Sebastian100% (1)
- L5 Exo in Ortho 2020Dokument9 SeitenL5 Exo in Ortho 2020Hassan MohamedNoch keine Bewertungen
- Classification of MalocclusionDokument79 SeitenClassification of MalocclusionMittali Vaibhav Sabnis50% (2)
- Canine ImpactionDokument10 SeitenCanine ImpactionPZ100% (1)
- Treatment Planning For Class I (Skeletal & Dental) MalocclusionDokument169 SeitenTreatment Planning For Class I (Skeletal & Dental) MalocclusionCyriac JohnNoch keine Bewertungen
- Orthodontics 1st Leture Difinitions 2021Dokument56 SeitenOrthodontics 1st Leture Difinitions 2021SRO oONoch keine Bewertungen
- Class II MalocclusionDokument192 SeitenClass II Malocclusionyounisismail935Noch keine Bewertungen
- On ImpactionDokument44 SeitenOn Impactionmesssi269Noch keine Bewertungen
- THE ORTHODONTIC ROADMAP: GUIDELINES FOR THE DIAGNOSIS AND TREATMENT OF ORTHODONTIC MALOCCLUSIONSVon EverandTHE ORTHODONTIC ROADMAP: GUIDELINES FOR THE DIAGNOSIS AND TREATMENT OF ORTHODONTIC MALOCCLUSIONSNoch keine Bewertungen
- Clinical Cases in Restorative and Reconstructive DentistryVon EverandClinical Cases in Restorative and Reconstructive DentistryBewertung: 5 von 5 Sternen5/5 (1)
- Reduction, Relocation and Splinting in Emergency Room (RASER)Von EverandReduction, Relocation and Splinting in Emergency Room (RASER)Noch keine Bewertungen
- Orthodontic Handbook for Dental AssistantsVon EverandOrthodontic Handbook for Dental AssistantsBewertung: 1 von 5 Sternen1/5 (1)
- Payment Receipt: To Validate This Document Using The QR Code, Please VisitDokument2 SeitenPayment Receipt: To Validate This Document Using The QR Code, Please Visitvinay kumarNoch keine Bewertungen
- SeriousadverseeventsformDokument2 SeitenSeriousadverseeventsformvinay kumarNoch keine Bewertungen
- Edit Check - A Critical Step To Ensure The Data Quality During Clinical TrialsDokument3 SeitenEdit Check - A Critical Step To Ensure The Data Quality During Clinical Trialsvinay kumarNoch keine Bewertungen
- PV QuestionsDokument7 SeitenPV Questionsvinay kumarNoch keine Bewertungen
- Addendum For Co ApplicantDokument2 SeitenAddendum For Co Applicantvinay kumarNoch keine Bewertungen
- Questions 1: Case 1Dokument3 SeitenQuestions 1: Case 1vinay kumarNoch keine Bewertungen
- Maxine Curry: Pharmacy TechnicianDokument2 SeitenMaxine Curry: Pharmacy Technicianvinay kumarNoch keine Bewertungen
- Thenedfo PVDokument25 SeitenThenedfo PVvinay kumarNoch keine Bewertungen
- Internship Certificate Template 2Dokument1 SeiteInternship Certificate Template 2vinay kumarNoch keine Bewertungen
- Optometry Exam Content and ReferencesDokument1 SeiteOptometry Exam Content and Referencesvinay kumarNoch keine Bewertungen
- MCQ Toxicology 2 PDFDokument16 SeitenMCQ Toxicology 2 PDFMarwaFakhro50% (6)
- Schs Loa UpdatedDokument1 SeiteSchs Loa UpdatedV.VNoch keine Bewertungen
- Pharma ToxicologyDokument24 SeitenPharma Toxicologyvinay kumarNoch keine Bewertungen
- Certificate PreviewDokument1 SeiteCertificate Previewvinay kumarNoch keine Bewertungen
- NHRA Licensing ProceduresDokument9 SeitenNHRA Licensing Proceduresvinay kumarNoch keine Bewertungen
- Al-HAJRY (Employment Form)Dokument2 SeitenAl-HAJRY (Employment Form)vinay kumarNoch keine Bewertungen
- JNTU-H Affiliated CollegesDokument20 SeitenJNTU-H Affiliated Collegesvinay kumarNoch keine Bewertungen
- نماذج اختبار الهيئة بالاجااباااتDokument68 Seitenنماذج اختبار الهيئة بالاجااباااتjawish80% (46)
- Argus AaascreensDokument4 SeitenArgus Aaascreensvinay kumarNoch keine Bewertungen
- Dosage Calculation PDFDokument23 SeitenDosage Calculation PDFKaren Ruste Villaluna-AbulenciaNoch keine Bewertungen
- MCQ Toxicology 2 PDFDokument16 SeitenMCQ Toxicology 2 PDFMarwaFakhro50% (6)
- SeriousadverseeventsformDokument2 SeitenSeriousadverseeventsformvinay kumarNoch keine Bewertungen
- HAAD Letter of AuthorizationDokument1 SeiteHAAD Letter of AuthorizationRenny M PNoch keine Bewertungen
- Basic Introduction To ICD-10-CMDokument54 SeitenBasic Introduction To ICD-10-CMcodingcertwriter100% (2)
- Dosage Calculation PDFDokument23 SeitenDosage Calculation PDFKaren Ruste Villaluna-AbulenciaNoch keine Bewertungen
- Pharma ToxicologyDokument24 SeitenPharma Toxicologyvinay kumarNoch keine Bewertungen
- Jurru MLT ExamDokument1 SeiteJurru MLT Examvinay kumar0% (1)
- New Registration for Pharm-D Application ChecklistDokument1 SeiteNew Registration for Pharm-D Application Checklistvinay kumarNoch keine Bewertungen
- 4D Printing With Programmable PolymersDokument36 Seiten4D Printing With Programmable PolymersdevanshNoch keine Bewertungen
- For The Moot Competition of Dr. Ram Manohar Lohia College of LawDokument11 SeitenFor The Moot Competition of Dr. Ram Manohar Lohia College of LawgreenrosenaikNoch keine Bewertungen
- Neuroscience Clerkship Teaching Vignettes on Cerebrovascular Disease and Changes in Mental StateDokument16 SeitenNeuroscience Clerkship Teaching Vignettes on Cerebrovascular Disease and Changes in Mental Statehippocamper100% (1)
- Forensic SerologyDokument13 SeitenForensic Serologyempress venus bonillaNoch keine Bewertungen
- Tarif Tindakan Paru PDPI 2017Dokument2 SeitenTarif Tindakan Paru PDPI 2017Yuyus Dwi PrasetiyoNoch keine Bewertungen
- Senior Sales Pharmaceuticals in Chicago IL Resume Pauline GrayDokument2 SeitenSenior Sales Pharmaceuticals in Chicago IL Resume Pauline GrayPaulineGrayNoch keine Bewertungen
- Case of Jennifer CagandahanDokument8 SeitenCase of Jennifer CagandahanArianneParalisanNoch keine Bewertungen
- Yoga - Art of CommunicationDokument221 SeitenYoga - Art of CommunicationMadhuri SathishNoch keine Bewertungen
- Jurnal Formulasi Krim Gentamisin SulfatDokument15 SeitenJurnal Formulasi Krim Gentamisin SulfatNandea Zulfana HendrawanNoch keine Bewertungen
- 04 Splintstrismus 140501160338 Phpapp02Dokument56 Seiten04 Splintstrismus 140501160338 Phpapp02hazeemmegahedNoch keine Bewertungen
- Arogyavardhini Vati - Benefits, Dosage, Ingredients, Side EffectsDokument3 SeitenArogyavardhini Vati - Benefits, Dosage, Ingredients, Side Effectsverna101Noch keine Bewertungen
- Efficacy of Cetirizine vs Loratadine for Allergic Rhinitis in Children (39Dokument9 SeitenEfficacy of Cetirizine vs Loratadine for Allergic Rhinitis in Children (39intan nabilah pratiwiNoch keine Bewertungen
- Guide to USP Dietary Supplement Monograph TitlesDokument36 SeitenGuide to USP Dietary Supplement Monograph TitlesYulian DyaswaraNoch keine Bewertungen
- Rhinoplasty (Nose Job) Surgery GuideDokument13 SeitenRhinoplasty (Nose Job) Surgery GuideMart UrsuNoch keine Bewertungen
- Organization and Composition of Body FluidsDokument7 SeitenOrganization and Composition of Body FluidsEVELYN ITZEL OCHOA VARGASNoch keine Bewertungen
- Duties and ResponsibilitiesDokument160 SeitenDuties and ResponsibilitiesKaushik Mandal67% (3)
- General Immunology University of Oradea Faculty ofDokument19 SeitenGeneral Immunology University of Oradea Faculty ofsacchinNoch keine Bewertungen
- 2 Segmentation PracticalDokument8 Seiten2 Segmentation PracticaldanxalreadyNoch keine Bewertungen
- Quick ASDAS-CRP Calculation Form: Name: - DateDokument2 SeitenQuick ASDAS-CRP Calculation Form: Name: - DateHüseyin YelkenNoch keine Bewertungen
- ATC CODE GROUPS AND SUBGROUPSDokument152 SeitenATC CODE GROUPS AND SUBGROUPSVishal Garg0% (1)
- Benefits of Breastfeeding for Child Survival and DevelopmentDokument7 SeitenBenefits of Breastfeeding for Child Survival and DevelopmentArfian Deny PNoch keine Bewertungen
- The Woman Who Tried To Murder Dr. King (The Izola Curry Case)Dokument2 SeitenThe Woman Who Tried To Murder Dr. King (The Izola Curry Case)Angelly V VelascoNoch keine Bewertungen
- Administering Enema: Low Enema - 30 CM (12 Inches)Dokument2 SeitenAdministering Enema: Low Enema - 30 CM (12 Inches)さいと フエンテ かずもとNoch keine Bewertungen
- Introduction To Medical TechnologyDokument18 SeitenIntroduction To Medical TechnologyChrissa Mae Tumaliuan Catindoy100% (1)
- Femoral Neck FracturesDokument8 SeitenFemoral Neck FracturesMorshed Mahbub AbirNoch keine Bewertungen
- Benefits of ChocolateDokument13 SeitenBenefits of ChocolateMohd Idris MohiuddinNoch keine Bewertungen
- ARC LASER: Catálogo - CLAS & OthersDokument54 SeitenARC LASER: Catálogo - CLAS & OthersAdolfo Garcia de GuadianaNoch keine Bewertungen
- Nervous System Endocrine System and Reproductive SystemDokument5 SeitenNervous System Endocrine System and Reproductive SystemMcdaryl Inmenzo Lleno50% (2)
- Indication, Contraindication and Complication of CircumcisionDokument16 SeitenIndication, Contraindication and Complication of CircumcisionRd manNoch keine Bewertungen
- Bahasa Inggeris Peralihan Pertengahan Tahun Paper 1 (2015)Dokument8 SeitenBahasa Inggeris Peralihan Pertengahan Tahun Paper 1 (2015)Nazurah Eryna100% (1)