Das könnte Ihnen auch gefallen
- Anatomy of The Eye - Dr. Lim-Cecilio (2022)Dokument3 SeitenAnatomy of The Eye - Dr. Lim-Cecilio (2022)Patricia ManaliliNoch keine Bewertungen
- OPTHA 1.1 ANATOMY OF THE EYEBALL - Dr. CapuchinoDokument4 SeitenOPTHA 1.1 ANATOMY OF THE EYEBALL - Dr. CapuchinoPatricia ManaliliNoch keine Bewertungen
- Open Angle GlaucomaDokument114 SeitenOpen Angle Glaucomahassan qureshiNoch keine Bewertungen
- Anatomy of The EyeballDokument3 SeitenAnatomy of The EyeballMary Joy OamilNoch keine Bewertungen
- Anatomy and Physio HandoutsDokument6 SeitenAnatomy and Physio HandoutsKoj LozadaNoch keine Bewertungen
- Renal PhsyiologyDokument9 SeitenRenal PhsyiologyRyan GosserNoch keine Bewertungen
- 08 - Glaucoma (English Ver.)Dokument85 Seiten08 - Glaucoma (English Ver.)Danny. JayNoch keine Bewertungen
- Ophthalmology Final TransDokument51 SeitenOphthalmology Final TransPatryk Dionisio100% (1)
- Ocular Drug DeliveryDokument3 SeitenOcular Drug DeliveryArmin ShafiNoch keine Bewertungen
- Pelvic Pain - Easy 5 Step Ultrasound EvaluationDokument1 SeitePelvic Pain - Easy 5 Step Ultrasound EvaluationFungai MuganhuNoch keine Bewertungen
- 15 Ed PDFDokument139 Seiten15 Ed PDFJohn Paul VillaflorNoch keine Bewertungen
- Lecture1-Human Eye SystemDokument29 SeitenLecture1-Human Eye SystemPrajakta KhobragadeNoch keine Bewertungen
- PSC CC NotesDokument10 SeitenPSC CC NotescassseeeyyyNoch keine Bewertungen
- GlaucomaDokument5 SeitenGlaucomaspringdingNoch keine Bewertungen
- Tumors of The Head and NeckDokument5 SeitenTumors of The Head and NeckMiguel CuevasNoch keine Bewertungen
- DISORDERS of The EYE and EARDokument8 SeitenDISORDERS of The EYE and EARAnna Carmela P. MelendezNoch keine Bewertungen
- Iris and Ciliary BodyDokument46 SeitenIris and Ciliary BodyPremaaloshineeThanabalNoch keine Bewertungen
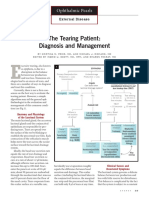
- The Tearing Patient: Diagnosis and Management: Ophthalmic PearlsDokument3 SeitenThe Tearing Patient: Diagnosis and Management: Ophthalmic PearlsAnonymous otk8ohj9Noch keine Bewertungen
- NotesDokument11 SeitenNotessofiaNoch keine Bewertungen
- Tonometry Clin OpDokument7 SeitenTonometry Clin OpVero VillamorNoch keine Bewertungen
- Chronological Survey of The Appearrance of Ocular StructuresDokument1 SeiteChronological Survey of The Appearrance of Ocular StructuresCJ DignosNoch keine Bewertungen
- Aesthetic Surgery BookDokument4 SeitenAesthetic Surgery BookmarizamoraNoch keine Bewertungen
- ED II Lens Camerae Bulbivitrous Body Accomodation TZSDokument25 SeitenED II Lens Camerae Bulbivitrous Body Accomodation TZSBojanaNoch keine Bewertungen
- 3 PDFDokument62 Seiten3 PDFDiwakesh C BNoch keine Bewertungen
- Aubf Lec Week 15Dokument7 SeitenAubf Lec Week 15Joanne RemolloNoch keine Bewertungen
- (OPTHA) Lec 5 - RetinaDokument5 Seiten(OPTHA) Lec 5 - RetinaPatricia ManaliliNoch keine Bewertungen
- Happ Finals Week 16-2Dokument7 SeitenHapp Finals Week 16-2qt potatoNoch keine Bewertungen
- Va L4 VempDokument27 SeitenVa L4 VempAfrina AzmiNoch keine Bewertungen
- Blood CollectionDokument4 SeitenBlood Collectionmgcapuyon8596valNoch keine Bewertungen
- VII - Urinary SystemDokument2 SeitenVII - Urinary SystemGael QuingNoch keine Bewertungen
- EENT NotesDokument12 SeitenEENT NotesMhae TabasaNoch keine Bewertungen
- Eyelids and Lacrimal ApparatusDokument6 SeitenEyelids and Lacrimal Apparatussarguss14Noch keine Bewertungen
- Telehealth Physical Exam: Eyes Neck Chest SkinDokument1 SeiteTelehealth Physical Exam: Eyes Neck Chest SkinYazeed QadadhaNoch keine Bewertungen
- Anatomy Rapid Express Notes EGurukul 2023Dokument56 SeitenAnatomy Rapid Express Notes EGurukul 2023Gaurav Prakash Gaurav100% (2)
- Arasitology: Intestinal AmoebaeDokument5 SeitenArasitology: Intestinal AmoebaeMa. Mil Adrianne PamaNoch keine Bewertungen
- Anaesthetic Management of Endoscopic Urologic Procedures: Universi Ty Medical Hospital Del HiDokument62 SeitenAnaesthetic Management of Endoscopic Urologic Procedures: Universi Ty Medical Hospital Del HiWafya RamschieNoch keine Bewertungen
- EyelidDokument10 SeitenEyelidrifqa rahmiNoch keine Bewertungen
- (OPHTHA) 2.05 Tearing - Rivera PDFDokument5 Seiten(OPHTHA) 2.05 Tearing - Rivera PDFRachel EstradaNoch keine Bewertungen
- Lecture 34 Kane Urinary System 4 Slides Per PageDokument8 SeitenLecture 34 Kane Urinary System 4 Slides Per Pageroselyn_061001Noch keine Bewertungen
- 2.drugs Acting On The EyeDokument19 Seiten2.drugs Acting On The EyeEman MohamedNoch keine Bewertungen
- L 01 Ocular AnatomyDokument13 SeitenL 01 Ocular Anatomydoni anandaNoch keine Bewertungen
- Evaluation of PupilDokument28 SeitenEvaluation of PupilArlinda Silva PrameswariNoch keine Bewertungen
- The Optic Nerve v.1Dokument22 SeitenThe Optic Nerve v.1Koj LozadaNoch keine Bewertungen
- Respiratory System HandoutDokument11 SeitenRespiratory System HandoutJohn Carlo SantiagoNoch keine Bewertungen
- Ocular ExaminationDokument2 SeitenOcular ExaminationMuhammad HaziqNoch keine Bewertungen
- VitreousDokument37 SeitenVitreousIhsanluthfi AbdillahNoch keine Bewertungen
- Ocular ExaminationDokument2 SeitenOcular ExaminationMuhammad HaziqNoch keine Bewertungen
- Slides 20 DuralVenousSinuses BrainAndNervousSystemDokument18 SeitenSlides 20 DuralVenousSinuses BrainAndNervousSystemNicole YatawaraNoch keine Bewertungen
- Assessing Cranial NerveDokument5 SeitenAssessing Cranial Nerve21-54405Noch keine Bewertungen
- (Ophtha) 7 - Diseases of The Conjunctiva, Cornea, and Sclera (2019)Dokument8 Seiten(Ophtha) 7 - Diseases of The Conjunctiva, Cornea, and Sclera (2019)NoreenNoch keine Bewertungen
- Special SensesDokument8 SeitenSpecial SensesGiane Qeirr Osias TimmalogNoch keine Bewertungen
- Opthal Summary AnatomyDokument14 SeitenOpthal Summary AnatomyNoman ButtNoch keine Bewertungen
- 2010 2physDokument12 Seiten2010 2physlahiruwan123Noch keine Bewertungen
- GlaucomaDokument52 SeitenGlaucomaIrfan SabirNoch keine Bewertungen
- Shanz - Ent 1.06 Facial Nerve and Traumatic Facial ParalysisDokument3 SeitenShanz - Ent 1.06 Facial Nerve and Traumatic Facial ParalysisPetrina XuNoch keine Bewertungen
- CSF and CSF CirculationDokument8 SeitenCSF and CSF CirculationLoredana M CurecheriuNoch keine Bewertungen
- Веб-страница 2Dokument1 SeiteВеб-страница 2Zalina IvanovaNoch keine Bewertungen
- Terapi CairanDokument81 SeitenTerapi CairanMarsa ZaidanNoch keine Bewertungen
- Histology and Histopathology of the Eye and Its AdnexaVon EverandHistology and Histopathology of the Eye and Its AdnexaNoch keine Bewertungen
- Moon2019 PDFDokument7 SeitenMoon2019 PDFGusti Zidni FahmiNoch keine Bewertungen
- Retinal DetachmentDokument2 SeitenRetinal DetachmentGusti Zidni FahmiNoch keine Bewertungen
- How To Detect Myopia in The Eye ClinicDokument2 SeitenHow To Detect Myopia in The Eye ClinicGusti Zidni FahmiNoch keine Bewertungen
- Bleph PDFDokument13 SeitenBleph PDFGusti Zidni FahmiNoch keine Bewertungen
- Nasolacrimal Duct Obstruction After Zygoma Fracture Reduction With Inferior Orbital Margin FixationDokument2 SeitenNasolacrimal Duct Obstruction After Zygoma Fracture Reduction With Inferior Orbital Margin FixationGusti Zidni FahmiNoch keine Bewertungen
- Distal Lakrimal Kanal T Kan KL Na e Lik Eden Lateral Nazal Duvar Patolojilerinin Incelenmesi (#180604) - 160005Dokument4 SeitenDistal Lakrimal Kanal T Kan KL Na e Lik Eden Lateral Nazal Duvar Patolojilerinin Incelenmesi (#180604) - 160005Gusti Zidni FahmiNoch keine Bewertungen
- Review Article Dietary Polyphenols in Age-Related Macular Degeneration: Protection Against Oxidative Stress and BeyondDokument14 SeitenReview Article Dietary Polyphenols in Age-Related Macular Degeneration: Protection Against Oxidative Stress and BeyondGusti Zidni FahmiNoch keine Bewertungen
- Diferensial Diagnosis Penyakit Nail Jamur: Table 1Dokument3 SeitenDiferensial Diagnosis Penyakit Nail Jamur: Table 1Gusti Zidni FahmiNoch keine Bewertungen
- Pathogenesis of Retinal Detachment PDFDokument11 SeitenPathogenesis of Retinal Detachment PDFGusti Zidni FahmiNoch keine Bewertungen
- Cryotherapy For Ocular Tumors-New Finger-Tip' Cryoprobes Provide A Wide Range of Uses and ApplicationsDokument2 SeitenCryotherapy For Ocular Tumors-New Finger-Tip' Cryoprobes Provide A Wide Range of Uses and ApplicationsGusti Zidni FahmiNoch keine Bewertungen
- Gangguan Non PsikotikDokument15 SeitenGangguan Non PsikotikGusti Zidni FahmiNoch keine Bewertungen
- Biecco Lawrie Ece Gec Reyrolle Burn Jyoti SwitchgearDokument18 SeitenBiecco Lawrie Ece Gec Reyrolle Burn Jyoti SwitchgearSharafat AliNoch keine Bewertungen
- X-Pruf Crystalcoat: Cementitious Crystalline Waterproof Coating For ConcreteDokument2 SeitenX-Pruf Crystalcoat: Cementitious Crystalline Waterproof Coating For ConcreteAmr RagabNoch keine Bewertungen
- Mechanical Interview Questions and Answers - Fluid MechanicsDokument2 SeitenMechanical Interview Questions and Answers - Fluid MechanicsannukiitNoch keine Bewertungen
- BS Pharmacy - ProspectusDokument9 SeitenBS Pharmacy - ProspectusDomz BucadNoch keine Bewertungen
- Top AttorneysDokument7 SeitenTop AttorneysArlington MagazineNoch keine Bewertungen
- Major Laishram Jyotin SinghDokument3 SeitenMajor Laishram Jyotin SinghSpongebob SquarepantsNoch keine Bewertungen
- Brief Psychological Interventions For Borderline Personality Disorder. A Systematic Review and Meta-Analysis of Randomised Controlled TrialsDokument9 SeitenBrief Psychological Interventions For Borderline Personality Disorder. A Systematic Review and Meta-Analysis of Randomised Controlled TrialsFELIPE ROJAS TRAVERSONoch keine Bewertungen
- XII Biology Practicals 2020-21 Without ReadingDokument32 SeitenXII Biology Practicals 2020-21 Without ReadingStylish HeroNoch keine Bewertungen
- Guide For Visual Inspection of Structural Concrete Building ComponentsDokument76 SeitenGuide For Visual Inspection of Structural Concrete Building ComponentsMazin AlwashNoch keine Bewertungen
- FPGA-based System For Heart Rate Monitoring PDFDokument12 SeitenFPGA-based System For Heart Rate Monitoring PDFkishorechiyaNoch keine Bewertungen
- Bituminous MixesDokument13 SeitenBituminous MixesRanjit SinghNoch keine Bewertungen
- Plumbing Design Calculation - North - Molino - PH1 - 5jun2017Dokument5 SeitenPlumbing Design Calculation - North - Molino - PH1 - 5jun2017Jazent Anthony RamosNoch keine Bewertungen
- Lending Policies of Indian BanksDokument47 SeitenLending Policies of Indian BanksProf Dr Chowdari Prasad80% (5)
- Matter and Change 2008 Chapter 14Dokument40 SeitenMatter and Change 2008 Chapter 14cattmy100% (1)
- D 7752Dokument6 SeitenD 7752Asep TheaNoch keine Bewertungen
- CBLMDokument37 SeitenCBLMDTVS Inc.Noch keine Bewertungen
- Norsok R 002Dokument186 SeitenNorsok R 002robson2015Noch keine Bewertungen
- Lesson 2.1 Earth As The Only Habitable PlanetDokument37 SeitenLesson 2.1 Earth As The Only Habitable Planetrosie sialanaNoch keine Bewertungen
- Chan vs. ChanDokument2 SeitenChan vs. ChanMmm GggNoch keine Bewertungen
- Azure Essentials: Module 5: Azure Cost Management and Service Level AgreementsDokument9 SeitenAzure Essentials: Module 5: Azure Cost Management and Service Level Agreementsrajagopalan19Noch keine Bewertungen
- Module 3 Passive Heating 8.3.18Dokument63 SeitenModule 3 Passive Heating 8.3.18Aman KashyapNoch keine Bewertungen
- Implementation Plan SLRPDokument6 SeitenImplementation Plan SLRPAngelina SantosNoch keine Bewertungen
- CSA11 CholelithiasisDokument3 SeitenCSA11 CholelithiasisBerlon LacsonNoch keine Bewertungen
- Motivational Interviewing (MI) Refers To ADokument5 SeitenMotivational Interviewing (MI) Refers To AJefri JohanesNoch keine Bewertungen
- digiPHONENT UG enDokument44 SeitendigiPHONENT UG enIrving Javier Leal OrtizNoch keine Bewertungen
- Research Article Effects of PH On The Shape of Alginate Particles and Its Release BehaviorDokument10 SeitenResearch Article Effects of PH On The Shape of Alginate Particles and Its Release BehaviorAmalia HanifaNoch keine Bewertungen
- Low Cholesterol DietDokument10 SeitenLow Cholesterol Dietkevintotz73Noch keine Bewertungen
- @9negros Occidental Vs BezoreDokument3 Seiten@9negros Occidental Vs BezoreSimeon SuanNoch keine Bewertungen
- Chrono Biology SeminarDokument39 SeitenChrono Biology SeminarSurabhi VishnoiNoch keine Bewertungen
- AJINOMOTO 2013 Ideal Amino Acid Profile For PigletsDokument28 SeitenAJINOMOTO 2013 Ideal Amino Acid Profile For PigletsFreddy Alexander Horna Morillo100% (1)