Das könnte Ihnen auch gefallen
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (400)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (74)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (345)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2259)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (121)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- Dose Rate Analysis of HDR Cobalt (Co-60) Afterloading Brachytherapy Unit Using Well Type Chamber Measurement MethodDokument9 SeitenDose Rate Analysis of HDR Cobalt (Co-60) Afterloading Brachytherapy Unit Using Well Type Chamber Measurement MethodGiner MaslebuNoch keine Bewertungen
- Uz Kontrasna SRDokument32 SeitenUz Kontrasna SRjovana100% (2)
- Pdfmergerfreecom Atlas Anatomi Manusia Sobotta Edisi 23 PDF OtomanuscomDokument2 SeitenPdfmergerfreecom Atlas Anatomi Manusia Sobotta Edisi 23 PDF OtomanuscomannisaNoch keine Bewertungen
- Webb S Physics of Medical Imagi - Flower M A PDFDokument829 SeitenWebb S Physics of Medical Imagi - Flower M A PDFjts99athotmaildotcomNoch keine Bewertungen
- Basda Catalogue 2014 PDFDokument24 SeitenBasda Catalogue 2014 PDFmsohrabieNoch keine Bewertungen
- Presentaion Key CompinesDokument32 SeitenPresentaion Key CompinesEng.Moayad HassanNoch keine Bewertungen
- Test Bank For Merrills Atlas of Radiographic Positioning and Procedures 3 Volume Set 14th Edition Bruce W Long Jeannean Hall Rollins Barbara J SmithDokument7 SeitenTest Bank For Merrills Atlas of Radiographic Positioning and Procedures 3 Volume Set 14th Edition Bruce W Long Jeannean Hall Rollins Barbara J SmithJack Williams100% (32)
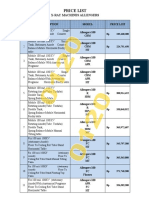
- Daftar Harga Allengers - 012020Dokument8 SeitenDaftar Harga Allengers - 012020Bintang Rejeki AlkesindoNoch keine Bewertungen
- The Medical Nuclear Physicist, Part of The Nuclear Medicine TeamDokument2 SeitenThe Medical Nuclear Physicist, Part of The Nuclear Medicine Teamgiulio141091Noch keine Bewertungen
- Conceptual FrameworkDokument7 SeitenConceptual FrameworkJelina G. IlaganNoch keine Bewertungen
- X Ray Tube EDokument8 SeitenX Ray Tube EAlberto Reyes Ambrosio100% (3)
- Rumpa Amornmarn, MD Honored With A Lifetime Achievement Award by P.O.W.E.R. and Will Be Featured On The Back Cover of P.O.W.E.R. MagazineDokument3 SeitenRumpa Amornmarn, MD Honored With A Lifetime Achievement Award by P.O.W.E.R. and Will Be Featured On The Back Cover of P.O.W.E.R. MagazinePR.comNoch keine Bewertungen
- Physics of Thermal Therapy: Fundamentals and Clinical ApplicationsDokument2 SeitenPhysics of Thermal Therapy: Fundamentals and Clinical ApplicationsarakbaeNoch keine Bewertungen
- HRCT LungsDokument10 SeitenHRCT Lungscatalyst1986Noch keine Bewertungen
- Icru 83Dokument112 SeitenIcru 83HanKethyanethNoch keine Bewertungen
- Image Weighting and ContrastDokument30 SeitenImage Weighting and ContrastNaseem Al tajerNoch keine Bewertungen
- Practical Differential Diagnosis For CT and Mri PDFDokument1 SeitePractical Differential Diagnosis For CT and Mri PDFAdriana VoicuNoch keine Bewertungen
- Hitachi HI VISION PreirusDokument7 SeitenHitachi HI VISION Preirusdaniyar9402Noch keine Bewertungen
- Carbon TransmitterDokument17 SeitenCarbon TransmitterSummit Testing & Calibration LaboratoryNoch keine Bewertungen
- Inventory Catalog: Buy / Sell /parts /serviceDokument12 SeitenInventory Catalog: Buy / Sell /parts /servicelaura islasNoch keine Bewertungen
- What Is RadiologyDokument11 SeitenWhat Is RadiologyMichaelNoch keine Bewertungen
- PTW PresentationDokument44 SeitenPTW PresentationGina RNoch keine Bewertungen
- Radiography: Radiography Is An Imaging TechniqueDokument52 SeitenRadiography: Radiography Is An Imaging TechniquePraveen PrasadNoch keine Bewertungen
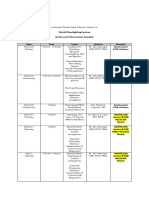
- Hybrid Moonlighting Seminar ScheduleDokument2 SeitenHybrid Moonlighting Seminar ScheduleSanielle Karla Garcia LorenzoNoch keine Bewertungen
- bayouth2003-MLC For Small Fields IMRTDokument8 Seitenbayouth2003-MLC For Small Fields IMRTJaviNoch keine Bewertungen
- IAEA Nuclear Medicine PublicationsDokument20 SeitenIAEA Nuclear Medicine PublicationsNéstor Raúl Arredondo Pérez100% (1)
- Physiology Biophysics and Biomedical EngDokument759 SeitenPhysiology Biophysics and Biomedical EngLUIS DAVID ROJAS CARDENAS100% (3)
- Laboratory ManualDokument7 SeitenLaboratory ManualTarekShabakaNoch keine Bewertungen
- 1.picture Archiving and Communication System (PACS)Dokument2 Seiten1.picture Archiving and Communication System (PACS)SamKris Guerrero MalasagaNoch keine Bewertungen