Das könnte Ihnen auch gefallen
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- Economic Cost Analysis of Hybrid Renewable Energy System Using HOMERDokument6 SeitenEconomic Cost Analysis of Hybrid Renewable Energy System Using HOMERAndiHilmySyahirNoch keine Bewertungen
- (Dwiky) A European View of Arc Flash Hazards and Electrical SafetyDokument7 Seiten(Dwiky) A European View of Arc Flash Hazards and Electrical SafetyAndiHilmySyahirNoch keine Bewertungen
- (Mahatir) Trend of International Safety StandardsDokument5 Seiten(Mahatir) Trend of International Safety StandardsAndiHilmySyahirNoch keine Bewertungen
- Elektronika Daya KuliahDokument50 SeitenElektronika Daya KuliahAndiHilmySyahirNoch keine Bewertungen
- Blavatsky y 2016Dokument7 SeitenBlavatsky y 2016AndiHilmySyahirNoch keine Bewertungen
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (400)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2259)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (74)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (345)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (121)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- Badoi A. 387318 PDFDokument53 SeitenBadoi A. 387318 PDFIrna P LestariNoch keine Bewertungen
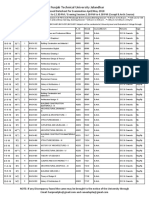
- Prposed Date Sheet Upload Web SiteDokument154 SeitenPrposed Date Sheet Upload Web SiteShaheer ShafatNoch keine Bewertungen
- EFDA - Guidelines For IVD Registration RequirementsDokument56 SeitenEFDA - Guidelines For IVD Registration RequirementsdawitNoch keine Bewertungen
- Moba Gaming Title ProposalDokument5 SeitenMoba Gaming Title ProposalJen PuetesNoch keine Bewertungen
- Sampling Technique and Data Collection Method in Qualitative ResearchDokument2 SeitenSampling Technique and Data Collection Method in Qualitative ResearchErica NapigkitNoch keine Bewertungen
- Aryannaprasadresume 11-11 WeeblyDokument2 SeitenAryannaprasadresume 11-11 Weeblyapi-235845755Noch keine Bewertungen
- Chapter One: Basic Statistical Concepts and NotationsDokument17 SeitenChapter One: Basic Statistical Concepts and NotationsCindyjune MarianoNoch keine Bewertungen
- Credit ManagementDokument9 SeitenCredit ManagementJayshreeDashaniNoch keine Bewertungen
- SCM201 - Ôn Quiz 2Dokument38 SeitenSCM201 - Ôn Quiz 2Quỳnh Lê DiễmNoch keine Bewertungen
- The Roots of Unfairness: The Black Swan in Arts and LiteratureDokument7 SeitenThe Roots of Unfairness: The Black Swan in Arts and LiteratureAlfian 'aaL' EikmanNoch keine Bewertungen
- It's Not Luck (1994) Is A Business: Novel Manufacturer Eliyahu M. GoldrattDokument2 SeitenIt's Not Luck (1994) Is A Business: Novel Manufacturer Eliyahu M. Goldrattpoish1Noch keine Bewertungen
- (Political Analysis) David Beetham - The Legitimation of Power-Palgrave Macmillan (2013) PDFDokument277 Seiten(Political Analysis) David Beetham - The Legitimation of Power-Palgrave Macmillan (2013) PDFdbkjasdkjahdkj100% (1)
- HR001123S0011Dokument57 SeitenHR001123S0011Ahmed LaajiliNoch keine Bewertungen
- PDF Eapp q1m3 Tehnques in Smmrizng Diff Acad Texts r5 - CompressDokument24 SeitenPDF Eapp q1m3 Tehnques in Smmrizng Diff Acad Texts r5 - CompressArjayNoch keine Bewertungen
- Identity Theory and Personality Theory: Mutual Relevance - Sheldon StrykerDokument24 SeitenIdentity Theory and Personality Theory: Mutual Relevance - Sheldon StrykerRemyNoch keine Bewertungen
- Rujukan ARDokument3 SeitenRujukan ARcrunx89Noch keine Bewertungen
- Internal Audit Sampling by IIADokument11 SeitenInternal Audit Sampling by IIAAndi Tri Jati86% (7)
- 1 Auditing 2 Chapter OneDokument7 Seiten1 Auditing 2 Chapter Onesamuel debebe100% (1)
- Tool 1 Example Risk Analysis For Financial StatementsDokument7 SeitenTool 1 Example Risk Analysis For Financial StatementsGretchen RicafrenteNoch keine Bewertungen
- HRM Selection 2018Dokument21 SeitenHRM Selection 2018Ayushi KavthankarNoch keine Bewertungen
- ExercisesDokument38 SeitenExercisesIrina StanciuNoch keine Bewertungen
- Handbook of Information 2017Dokument302 SeitenHandbook of Information 2017Shama ParveenNoch keine Bewertungen
- Margaret Mead (1901-1978)Dokument19 SeitenMargaret Mead (1901-1978)แคน แดนอีสานNoch keine Bewertungen
- 1 Defining Social Sciences PDFDokument2 Seiten1 Defining Social Sciences PDFCarla villalva100% (2)
- Mini Project ReportDokument25 SeitenMini Project ReportTejas NitnavareNoch keine Bewertungen
- Brainstorming For Research TopicsDokument18 SeitenBrainstorming For Research TopicsMa. Aiza SantosNoch keine Bewertungen
- Mat 2377 Final 2011Dokument12 SeitenMat 2377 Final 2011David LinNoch keine Bewertungen
- Micro OB Syllabus - 18-20Dokument2 SeitenMicro OB Syllabus - 18-20Abhishek rajNoch keine Bewertungen
- Excel For Statistical Data AnalysisDokument54 SeitenExcel For Statistical Data AnalysisLords PorseenaNoch keine Bewertungen
- Sandra J. Savignon - Interpreting Communicative Language Teaching - Contexts and Concerns in Teacher Education (2002) PDFDokument238 SeitenSandra J. Savignon - Interpreting Communicative Language Teaching - Contexts and Concerns in Teacher Education (2002) PDFDunia Duval50% (2)