Das könnte Ihnen auch gefallen
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- File IndexDokument1 SeiteFile IndexmaheshNoch keine Bewertungen
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- My ActivitiesDokument9 SeitenMy ActivitiesmaheshNoch keine Bewertungen
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- File IndexDokument1 SeiteFile IndexmaheshNoch keine Bewertungen
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
- Sample Cover LettersDokument8 SeitenSample Cover LettersImmad Uddin KhanNoch keine Bewertungen
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (400)
- 11 - 8 Steps To Success in Maintenance Planning and Scheduling PDFDokument42 Seiten11 - 8 Steps To Success in Maintenance Planning and Scheduling PDFmsaad19103564100% (2)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- 11 - 8 Steps To Success in Maintenance Planning and Scheduling PDFDokument42 Seiten11 - 8 Steps To Success in Maintenance Planning and Scheduling PDFmsaad19103564100% (2)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- Out of ServiceDokument2 SeitenOut of ServicemaheshNoch keine Bewertungen
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- Switch OFF The Power Supply of The MachineDokument2 SeitenSwitch OFF The Power Supply of The MachinemaheshNoch keine Bewertungen
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
- Quotation: Mextech Technologies India PVT LTDDokument1 SeiteQuotation: Mextech Technologies India PVT LTDmaheshNoch keine Bewertungen
- Backfill SpecificationDokument5 SeitenBackfill SpecificationRrsNoch keine Bewertungen
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- Audit ProcessDokument4 SeitenAudit ProcessmaheshNoch keine Bewertungen
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (74)
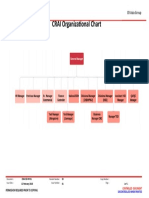
- 5.b) Total Organizational ChartDokument1 Seite5.b) Total Organizational ChartmaheshNoch keine Bewertungen
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- Cover Letter UkDokument1 SeiteCover Letter UkNayan MallickNoch keine Bewertungen
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- Quote 1341 PDFDokument2 SeitenQuote 1341 PDFmaheshNoch keine Bewertungen
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (344)
- Astm A380Dokument1 SeiteAstm A380maheshNoch keine Bewertungen
- New Doc 2019-10-31 11.27.12Dokument1 SeiteNew Doc 2019-10-31 11.27.12maheshNoch keine Bewertungen
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2259)
- Eliminating Inert Entry For CatalystDokument2 SeitenEliminating Inert Entry For CatalystAndri SaputraNoch keine Bewertungen
- Sr. No. Description Serial No. 1Dokument2 SeitenSr. No. Description Serial No. 1maheshNoch keine Bewertungen
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- Asme B16.48-2010 PDFDokument56 SeitenAsme B16.48-2010 PDFSleh Fki80% (5)
- Vending Machine Cleaning InstructionDokument1 SeiteVending Machine Cleaning InstructionmaheshNoch keine Bewertungen
- Government PolytechnicDokument2 SeitenGovernment PolytechnicmaheshNoch keine Bewertungen
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- Eye Test CertificateDokument1 SeiteEye Test CertificatemaheshNoch keine Bewertungen
- Dispatch DateDokument2 SeitenDispatch DatemaheshNoch keine Bewertungen
- V65 N2 P3 C822 KafaliDokument16 SeitenV65 N2 P3 C822 KafalimaheshNoch keine Bewertungen
- M14 TM 9-1005-223-34Dokument64 SeitenM14 TM 9-1005-223-34Daniel WilliamsNoch keine Bewertungen
- MAPEI Webinar Presentation BS 091818Dokument39 SeitenMAPEI Webinar Presentation BS 091818AamirShabbirNoch keine Bewertungen
- Börger RLP (Simplicity) PDFDokument8 SeitenBörger RLP (Simplicity) PDFMilena Lemus FonsecaNoch keine Bewertungen
- Corrosion RingsDokument1 SeiteCorrosion RingsAnonymous JMuM0E5YONoch keine Bewertungen
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (121)
- Disperse Manual PDFDokument207 SeitenDisperse Manual PDFNishanth MenonNoch keine Bewertungen
- K3Dokument5 SeitenK3Dani SetiawanNoch keine Bewertungen
- Salt AnalysisDokument10 SeitenSalt Analysisamrita girishNoch keine Bewertungen
- A New Chemical Criterion For The Quality Control of Fish: Trimethylamine/Total Volatile Basic Nitrogen (%)Dokument5 SeitenA New Chemical Criterion For The Quality Control of Fish: Trimethylamine/Total Volatile Basic Nitrogen (%)Edwin Cárdenas GamarraNoch keine Bewertungen
- Balabanoff F19Dokument11 SeitenBalabanoff F19asoooomi_11Noch keine Bewertungen
- Checklist of E/OHS Activities For Asbestos Management: Name of Publication DateDokument20 SeitenChecklist of E/OHS Activities For Asbestos Management: Name of Publication DateidahssNoch keine Bewertungen
- Law of Errors: Errors in Measurement SystemDokument6 SeitenLaw of Errors: Errors in Measurement Systemrodrigo100% (1)
- Biochemistry of Connective Tissue DentistrykopptxDokument97 SeitenBiochemistry of Connective Tissue DentistrykopptxAbdullah Khalid VirkNoch keine Bewertungen
- En - 0122 8706 Ccta 20 01 00149Dokument10 SeitenEn - 0122 8706 Ccta 20 01 00149mrcariNoch keine Bewertungen
- Removal of Methyl Orange Dye From Textile Effluent Using Adsorption On Chitosan Hydrogel BeadsDokument8 SeitenRemoval of Methyl Orange Dye From Textile Effluent Using Adsorption On Chitosan Hydrogel BeadsESSENCE - International Journal for Environmental Rehabilitation and ConservaionNoch keine Bewertungen
- Zaikov CVDokument3 SeitenZaikov CVArif SantosoNoch keine Bewertungen
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- MPS ITP Bare Pipe - PT Sari Dumai Oleo (Signed SAP)Dokument30 SeitenMPS ITP Bare Pipe - PT Sari Dumai Oleo (Signed SAP)Alfian ImaduddinNoch keine Bewertungen
- Gaussian 03 Winodws TutorialDokument4 SeitenGaussian 03 Winodws Tutorialfernandojardim12Noch keine Bewertungen
- (SLIDES) Concrete Durability - An Industry Perspective - Vijaykulkarni PDFDokument80 Seiten(SLIDES) Concrete Durability - An Industry Perspective - Vijaykulkarni PDFO SNoch keine Bewertungen
- Action Potentials and Synapses HandoutsDokument6 SeitenAction Potentials and Synapses HandoutsKelly TrainorNoch keine Bewertungen
- Stable Solid Deodorant Product Grape Fruit1Dokument15 SeitenStable Solid Deodorant Product Grape Fruit1sabunbeningNoch keine Bewertungen
- Growth Promotion Test Guide For Media Used in Sterility TestsDokument5 SeitenGrowth Promotion Test Guide For Media Used in Sterility Testshoria96Noch keine Bewertungen
- Indian School Muscat: Senior Section Department of ChemistryDokument1 SeiteIndian School Muscat: Senior Section Department of ChemistryRitaNoch keine Bewertungen
- EquilibriaDokument57 SeitenEquilibriaRaishaSheikh04Noch keine Bewertungen
- Calculation of Pipe Reinforcement ASME B31 3Dokument5 SeitenCalculation of Pipe Reinforcement ASME B31 3Umar Aslam0% (1)
- Transpiration ResourceDokument33 SeitenTranspiration ResourceGgdhdgsg KdhahshhNoch keine Bewertungen
- World Atmospheric CO2, Its 14C Specific Activity,.2Dokument15 SeitenWorld Atmospheric CO2, Its 14C Specific Activity,.2Anonymous yE2LIYBNoch keine Bewertungen
- Compressible Fluid FlowDokument41 SeitenCompressible Fluid FlowSushil Thakkar100% (1)
- Sol-Gel Synthesis and Structure of Cordieritetialite Glass-CeramicsDokument6 SeitenSol-Gel Synthesis and Structure of Cordieritetialite Glass-CeramicsahadsajjadiNoch keine Bewertungen
- 985 22647-R02 Installation Manual ORCA Offshore Part1Dokument21 Seiten985 22647-R02 Installation Manual ORCA Offshore Part1dumpuu100% (1)
- Hydration of C3A With Calcium Sulfate Alone and in The Presence of Calcium SilicateDokument154 SeitenHydration of C3A With Calcium Sulfate Alone and in The Presence of Calcium SilicatememorphNoch keine Bewertungen
- AP® Chemistry Crash Course, For the 2020 Exam, Book + Online: Get a Higher Score in Less TimeVon EverandAP® Chemistry Crash Course, For the 2020 Exam, Book + Online: Get a Higher Score in Less TimeBewertung: 5 von 5 Sternen5/5 (1)
- Periodic Tales: A Cultural History of the Elements, from Arsenic to ZincVon EverandPeriodic Tales: A Cultural History of the Elements, from Arsenic to ZincBewertung: 3.5 von 5 Sternen3.5/5 (137)
- Is That a Fact?: Frauds, Quacks, and the Real Science of Everyday LifeVon EverandIs That a Fact?: Frauds, Quacks, and the Real Science of Everyday LifeBewertung: 5 von 5 Sternen5/5 (4)
- The Nature of Drugs Vol. 1: History, Pharmacology, and Social ImpactVon EverandThe Nature of Drugs Vol. 1: History, Pharmacology, and Social ImpactBewertung: 5 von 5 Sternen5/5 (5)