Das könnte Ihnen auch gefallen
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (344)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (121)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (399)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (73)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- Regents Homeostasis and EnzymesDokument5 SeitenRegents Homeostasis and Enzymesapi-3031203990% (1)
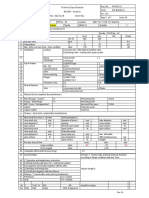
- SLR Strainer Data SheetDokument7 SeitenSLR Strainer Data SheetKailas NimbalkarNoch keine Bewertungen
- tmpA3C2 TMPDokument11 SeitentmpA3C2 TMPFrontiersNoch keine Bewertungen
- Wear Debris AnalysisDokument2 SeitenWear Debris Analysisthoma111sNoch keine Bewertungen
- 0423a ASKIN XFLAM Performance Panel Roofing-1Dokument11 Seiten0423a ASKIN XFLAM Performance Panel Roofing-1MacNoch keine Bewertungen
- Ceramic Tile Fixing StatementDokument5 SeitenCeramic Tile Fixing StatementAmit KhazanchiNoch keine Bewertungen
- Chemistry Uttam Chapter Paper SolutionsDokument175 SeitenChemistry Uttam Chapter Paper Solutionsswanandbarapatre12Noch keine Bewertungen
- Chem2 Lesson 1 - Kinetic Molecular Model of Liquids and SolidsDokument8 SeitenChem2 Lesson 1 - Kinetic Molecular Model of Liquids and SolidsCarl EscalaNoch keine Bewertungen
- Salting-Out Crystallisation Using NH Ina Laboratory-Scale Gas Lift ReactorDokument10 SeitenSalting-Out Crystallisation Using NH Ina Laboratory-Scale Gas Lift ReactorChester LowreyNoch keine Bewertungen
- Hyperbaric Oxygen TherapyDokument7 SeitenHyperbaric Oxygen Therapy18juni1995Noch keine Bewertungen
- Masel Catalog - WiresDokument30 SeitenMasel Catalog - WiresOrtho OrganizersNoch keine Bewertungen
- Exercises: Not One of The Possible Answers ListedDokument12 SeitenExercises: Not One of The Possible Answers ListedSarah ChoiNoch keine Bewertungen
- S.No. Type Medicine NameDokument6 SeitenS.No. Type Medicine Namered petalsNoch keine Bewertungen
- Biology - Chromatography Lab ReportDokument7 SeitenBiology - Chromatography Lab ReportJuana TestNoch keine Bewertungen
- 3 PRE BOARD GENERAL EDUCATION Some College StudentsDokument14 Seiten3 PRE BOARD GENERAL EDUCATION Some College StudentsMary-Rose CasuyonNoch keine Bewertungen
- Lampara de Fotocurado Bluephase MCDokument72 SeitenLampara de Fotocurado Bluephase MCErika PinillosNoch keine Bewertungen
- Fisher EZ Sliding - Stem Control Valve: The Easy - Et Valve FamilyDokument20 SeitenFisher EZ Sliding - Stem Control Valve: The Easy - Et Valve FamilyAlberto GuillenNoch keine Bewertungen
- Waste Minimization by Process Modification: Original ContributionDokument12 SeitenWaste Minimization by Process Modification: Original ContributionVirginiaNoch keine Bewertungen
- IB-DU1000 Metal-Enclosed Bus PDFDokument12 SeitenIB-DU1000 Metal-Enclosed Bus PDFdestro57Noch keine Bewertungen
- Structure of Atoms-11th Cbse Text AnswersDokument33 SeitenStructure of Atoms-11th Cbse Text AnswersKalai VananNoch keine Bewertungen
- "Promotional Activity of RCF Fertilizers Through Print Media (RCF Sheti PatrikaDokument26 Seiten"Promotional Activity of RCF Fertilizers Through Print Media (RCF Sheti PatrikagirishtorawaneNoch keine Bewertungen
- Materials and Design: Ehab A. El-Danaf, Magdy M. El-Rayes, Mahmoud S. SolimanDokument6 SeitenMaterials and Design: Ehab A. El-Danaf, Magdy M. El-Rayes, Mahmoud S. Solimankamal touilebNoch keine Bewertungen
- (En GB) DBE 821 - 1.00Dokument7 Seiten(En GB) DBE 821 - 1.00Enio Miguel Cano LimaNoch keine Bewertungen
- Mixture RequirementsDokument11 SeitenMixture Requirementsrajesh0% (1)
- Agricultural Control Chemicals (1950)Dokument277 SeitenAgricultural Control Chemicals (1950)Sveti JeronimNoch keine Bewertungen
- PC 0189 - Heat Resisting Silicone Aluminium Paint - Apcotherm 540Dokument3 SeitenPC 0189 - Heat Resisting Silicone Aluminium Paint - Apcotherm 540onshore purchase100% (1)
- National Waste Management Strategy 2019-2023Dokument64 SeitenNational Waste Management Strategy 2019-2023Chikondi KanamaNoch keine Bewertungen
- Betadex Sulfobutyl Ether SodiumDokument11 SeitenBetadex Sulfobutyl Ether SodiumLeidy GonzalezNoch keine Bewertungen
- Antinociceptive Activity of Buddleja Globosa (Matico)Dokument6 SeitenAntinociceptive Activity of Buddleja Globosa (Matico)alinumlNoch keine Bewertungen