Das könnte Ihnen auch gefallen
- Scope of The Problem: DefinitionsDokument34 SeitenScope of The Problem: DefinitionsDecky AndreaNoch keine Bewertungen
- Optimización HemodinámicaDokument9 SeitenOptimización HemodinámicaConstanza Casas BaezNoch keine Bewertungen
- Dr. Renny - Slide Webinar IDENTIA&PPKDokument41 SeitenDr. Renny - Slide Webinar IDENTIA&PPKClarissa HartawanNoch keine Bewertungen
- CUIDADOS PALIATIVOS-Aguilar y Otros-El Dolor en El Enfermo Hematológico Cuidados Paliativos IntegralesDokument13 SeitenCUIDADOS PALIATIVOS-Aguilar y Otros-El Dolor en El Enfermo Hematológico Cuidados Paliativos IntegralesLázaro MircovichNoch keine Bewertungen
- Transfusion Ternate 2019. LugyantiDokument28 SeitenTransfusion Ternate 2019. LugyantiAi SidiumarNoch keine Bewertungen
- Outcome of Patients Undergoing Amputation For Diabetic Foot UlcerDokument4 SeitenOutcome of Patients Undergoing Amputation For Diabetic Foot UlcerrischaNoch keine Bewertungen
- Risk Factors and Surgical Management of Incisional HerniasDokument5 SeitenRisk Factors and Surgical Management of Incisional HerniasRazvan UngureanuNoch keine Bewertungen
- Pressure Ulcer Prevalence and Quality of Care in Indonesian Stroke PatientsDokument5 SeitenPressure Ulcer Prevalence and Quality of Care in Indonesian Stroke Patientsifi medanNoch keine Bewertungen
- Cirugi A Espan Ola: Approach and Management of Traumatic Retroperitoneal InjuriesDokument10 SeitenCirugi A Espan Ola: Approach and Management of Traumatic Retroperitoneal InjuriesGrace TeweNoch keine Bewertungen
- 2 Atypical Ulcers 2019Dokument7 Seiten2 Atypical Ulcers 2019castillojessNoch keine Bewertungen
- Pleural EffusionDokument12 SeitenPleural EffusionDORINNE KINDAONoch keine Bewertungen
- Community Acquired PneumoniaDokument6 SeitenCommunity Acquired PneumoniaJia-PeiWuNoch keine Bewertungen
- Ma 70 379Dokument5 SeitenMa 70 379Sonia khanNoch keine Bewertungen
- ITP 11-9-20-dr - WidiDokument39 SeitenITP 11-9-20-dr - WidiWenny TanyawanNoch keine Bewertungen
- 176 FullDokument6 Seiten176 FullAlexisNoch keine Bewertungen
- Absceso y Fistula AnalDokument24 SeitenAbsceso y Fistula AnalSinue PumaNoch keine Bewertungen
- Cancer Cancer Pain and The Cancer Pain IDokument3 SeitenCancer Cancer Pain and The Cancer Pain Iab.ag.ay.222Noch keine Bewertungen
- Prolo 2Dokument8 SeitenProlo 2Joko JokoNoch keine Bewertungen
- Randomized Clinical Study To Compare Negative Pressure Wound Therapy With Simultaneous Saline Irrigation and Traditional Negative Pressure Wound Therapy For Complex Foot InfectionsDokument8 SeitenRandomized Clinical Study To Compare Negative Pressure Wound Therapy With Simultaneous Saline Irrigation and Traditional Negative Pressure Wound Therapy For Complex Foot InfectionsAsmat BurhanNoch keine Bewertungen
- The Hazards of Hospitalization : Classic PaperDokument7 SeitenThe Hazards of Hospitalization : Classic Paperujangketul62Noch keine Bewertungen
- Whyismypatient Bleedingorbruising?: Natalia Rydz,, Paula D. JamesDokument24 SeitenWhyismypatient Bleedingorbruising?: Natalia Rydz,, Paula D. Jamescamila perillaNoch keine Bewertungen
- Review of Internal HerniasDokument15 SeitenReview of Internal HerniassavingtaviaNoch keine Bewertungen
- Eficacia y Seguridad Del Sevoflurano en Ulceras CronicasDokument7 SeitenEficacia y Seguridad Del Sevoflurano en Ulceras CronicasYolis MirandaNoch keine Bewertungen
- The Assessment and Management of Acute and Chronic Cancer Pain SyndromesDokument6 SeitenThe Assessment and Management of Acute and Chronic Cancer Pain SyndromeszhuangemrysNoch keine Bewertungen
- Nigam A Et Al. Int Surg J. 2020 MayDokument6 SeitenNigam A Et Al. Int Surg J. 2020 MaydrpklalNoch keine Bewertungen
- Lary 28860Dokument5 SeitenLary 28860TitinNoch keine Bewertungen
- 29 e 9Dokument8 Seiten29 e 9Levi AckermanNoch keine Bewertungen
- 5 6+originalDokument2 Seiten5 6+originalnkoamartin8Noch keine Bewertungen
- Assessment and management of pressure soresDokument19 SeitenAssessment and management of pressure soresugandanursingschool bwindi100% (1)
- Incidence of Fistula After Management of Perianal AbscessDokument15 SeitenIncidence of Fistula After Management of Perianal AbscessenitaNoch keine Bewertungen
- Pressure Ulcer Assessment and Treatment (PDFDrive)Dokument88 SeitenPressure Ulcer Assessment and Treatment (PDFDrive)Amna AliNoch keine Bewertungen
- 10 1056@NEJMcpc1516450 PDFDokument7 Seiten10 1056@NEJMcpc1516450 PDFCarolina JaramilloNoch keine Bewertungen
- Rajivgandhi University of Health Sciences Bangalore, KarnatakaDokument20 SeitenRajivgandhi University of Health Sciences Bangalore, Karnatakafrank.buttigiegNoch keine Bewertungen
- Case 8-2017 - A 39-Year-Old Zimbabwean Man With A Severe HeadacheDokument7 SeitenCase 8-2017 - A 39-Year-Old Zimbabwean Man With A Severe HeadacheRoberto López Mata100% (1)
- Review of Hemorrhoid Disease: Presentation and Management: Zhifei Sun, MD John Migaly, MDDokument8 SeitenReview of Hemorrhoid Disease: Presentation and Management: Zhifei Sun, MD John Migaly, MDRB M ESNoch keine Bewertungen
- Nieto Et Al - Monitoração Hemodinâmica PlestimografiaDokument9 SeitenNieto Et Al - Monitoração Hemodinâmica PlestimografiaHarrisonNoch keine Bewertungen
- Jurnal Pendukung Data DisminoreDokument8 SeitenJurnal Pendukung Data DisminorePuput AnggarNoch keine Bewertungen
- Adenomyosis A Sonographic DiagnosisDokument14 SeitenAdenomyosis A Sonographic DiagnosisHelioNoch keine Bewertungen
- Managing Retroperitoneal HematomasDokument6 SeitenManaging Retroperitoneal HematomasEdwin OkonNoch keine Bewertungen
- Nejmcp 1905181Dokument9 SeitenNejmcp 1905181Hany ZutanNoch keine Bewertungen
- Derrame MalignoDokument9 SeitenDerrame MalignoMARIA NEGRETE MOSCOTENoch keine Bewertungen
- Orthopedic MedicineDokument13 SeitenOrthopedic MedicineAnonymous kdBDppigENoch keine Bewertungen
- Pressure Ulcers in Four Indonesian Hospitals: Prevalence, Patient Characteristics, Ulcer Characteristics, Prevention and TreatmentDokument11 SeitenPressure Ulcers in Four Indonesian Hospitals: Prevalence, Patient Characteristics, Ulcer Characteristics, Prevention and Treatmentpka25Noch keine Bewertungen
- Symptom Management Guidelines: Care of Malignant WoundsDokument7 SeitenSymptom Management Guidelines: Care of Malignant WoundsPatrico Rillah Setiawan100% (1)
- Thebasicsofhealthcare: Lesson5:U.S.Healthcaresystem LearningobjectivesDokument9 SeitenThebasicsofhealthcare: Lesson5:U.S.Healthcaresystem LearningobjectivesKibegwa MoriaNoch keine Bewertungen
- Dermatology: Continuing Medical EducationDokument22 SeitenDermatology: Continuing Medical EducationCynthia FloraNoch keine Bewertungen
- Diabetic (Neuropathic) Ulcers: Ulcer AssessmentDokument4 SeitenDiabetic (Neuropathic) Ulcers: Ulcer AssessmentGladys MainaNoch keine Bewertungen
- FGI BF ClearancesPatientsOfSize March2016Dokument63 SeitenFGI BF ClearancesPatientsOfSize March2016alvychuNoch keine Bewertungen
- Prevention of DVT & PE-1Dokument12 SeitenPrevention of DVT & PE-1arongeremewNoch keine Bewertungen
- 394 FullDokument7 Seiten394 FullkemashabibiNoch keine Bewertungen
- Ecos 11-13sDokument3 SeitenEcos 11-13scynthia narvy100% (1)
- Burden of Serious Harms From Diagnostic Error in The USADokument12 SeitenBurden of Serious Harms From Diagnostic Error in The USACBS PhiladelphiaNoch keine Bewertungen
- SepsisDokument14 SeitenSepsislengkong100% (9)
- Pneumonia ElderlyDokument13 SeitenPneumonia ElderlyAndreaNoch keine Bewertungen
- Acceptability of Gastrostomy Feeding in MalaysiaDokument2 SeitenAcceptability of Gastrostomy Feeding in Malaysiangoth678Noch keine Bewertungen
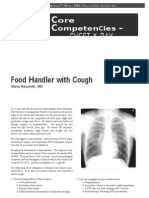
- Chest X-Ray: Food Handler With CoughDokument6 SeitenChest X-Ray: Food Handler With CoughSamuel Pola Karta SembiringNoch keine Bewertungen
- Pressure Ulcers: The Case For Improving Prevention and Management in Australian Health Care SettingsDokument10 SeitenPressure Ulcers: The Case For Improving Prevention and Management in Australian Health Care Settingsmahadabrata21Noch keine Bewertungen
- Elective Splenectomy: DisordersDokument5 SeitenElective Splenectomy: DisordersBogdan TrandafirNoch keine Bewertungen
- Pressure Ulcers in the Aging Population: A Guide for CliniciansVon EverandPressure Ulcers in the Aging Population: A Guide for CliniciansDavid R. Thomas, MDNoch keine Bewertungen
- Inflammatory Dermatopathology: A Pathologist's Survival GuideVon EverandInflammatory Dermatopathology: A Pathologist's Survival GuideNoch keine Bewertungen
- ADA Patient History Form (2019 - 01 - 09 22 - 31 - 23 UTC)Dokument1 SeiteADA Patient History Form (2019 - 01 - 09 22 - 31 - 23 UTC)sidney drecotteNoch keine Bewertungen
- Project Preposal 1988Dokument13 SeitenProject Preposal 1988sidney drecotteNoch keine Bewertungen
- GMFCS E&R Between 6th and 12th Birthday: Descriptors and IllustrationsDokument3 SeitenGMFCS E&R Between 6th and 12th Birthday: Descriptors and Illustrationssidney drecotteNoch keine Bewertungen
- Clinical Guidlines of Stroke Management 2017Dokument56 SeitenClinical Guidlines of Stroke Management 2017sidney drecotteNoch keine Bewertungen
- EPIDEMIOLOGY: Prevention and Treatment: EstimatesDokument7 SeitenEPIDEMIOLOGY: Prevention and Treatment: Estimatessidney drecotteNoch keine Bewertungen
- Clinical Guidelines OverviewDokument36 SeitenClinical Guidelines OverviewFatahilah MfNoch keine Bewertungen
- Handover Report: What Is The Handover Report and What Is Its PurposeDokument2 SeitenHandover Report: What Is The Handover Report and What Is Its Purposemaidieulinh156Noch keine Bewertungen
- Special Consideration Medical CertificateDokument1 SeiteSpecial Consideration Medical Certificatesidney drecotteNoch keine Bewertungen
- Concussion Position Statement 2016Dokument30 SeitenConcussion Position Statement 2016sidney drecotteNoch keine Bewertungen
- Practitioner Manual Wheelchairs & ScootersDokument22 SeitenPractitioner Manual Wheelchairs & Scooterssidney drecotteNoch keine Bewertungen
- Standard lofty garage kits include full length upper floor and drop down stair ladderDokument1 SeiteStandard lofty garage kits include full length upper floor and drop down stair laddersidney drecotteNoch keine Bewertungen
- BeginnerBoxerToolkit v1.0Dokument67 SeitenBeginnerBoxerToolkit v1.0Cavalera MaxNoch keine Bewertungen
- Standards For Wound Prevention and Management 2016Dokument66 SeitenStandards For Wound Prevention and Management 2016sidney drecotteNoch keine Bewertungen
- BetterLiving WheeledWalker AllTerrain 2015Dokument2 SeitenBetterLiving WheeledWalker AllTerrain 2015sidney drecotteNoch keine Bewertungen
- 2012 AWMA Pan Pacific Guidelines PDFDokument124 Seiten2012 AWMA Pan Pacific Guidelines PDFsidney drecotteNoch keine Bewertungen
- 2012 AWMA Pan Pacific GuidelinesDokument124 Seiten2012 AWMA Pan Pacific Guidelinessidney drecotteNoch keine Bewertungen
- Verdict SearchDokument32 SeitenVerdict Searchlaw365Noch keine Bewertungen
- Cv. Dr. Saldy YusufDokument6 SeitenCv. Dr. Saldy YusufMuhammad FaturrahmanNoch keine Bewertungen
- Sunrise Medical MattressesDokument4 SeitenSunrise Medical MattressesJulie SavoieNoch keine Bewertungen
- Complete Guide to Patient Positioning BasicsDokument13 SeitenComplete Guide to Patient Positioning BasicsAbriann Vince ImpenioNoch keine Bewertungen
- Nursing Care Plan Risk For Skin BreakdownDokument3 SeitenNursing Care Plan Risk For Skin BreakdownShelli Miller Pryor82% (11)
- DocuNotes Clinical Pocket Guide To Effective ChartingDokument203 SeitenDocuNotes Clinical Pocket Guide To Effective ChartingShirlyn Ares Navarro96% (47)
- Impaired Skin Integrity NCPDokument4 SeitenImpaired Skin Integrity NCPClint DelacruzNoch keine Bewertungen
- Body Mechanics and Transferring PatientDokument57 SeitenBody Mechanics and Transferring PatientRhenier S. Ilado100% (2)
- Modalities & Wound CareDokument0 SeitenModalities & Wound CareAndika Laksmana KurniadiNoch keine Bewertungen
- Operations/Maintenance Manual: Proform ™Dokument134 SeitenOperations/Maintenance Manual: Proform ™mohamed hegazyNoch keine Bewertungen
- Pressure Ulcers and Hydrocolloids Made EasyDokument6 SeitenPressure Ulcers and Hydrocolloids Made EasyJefferson AlexandreNoch keine Bewertungen
- Sampling sizeFull sampling of all patients with suspected thrombophlebitisand catheter associated blood stream infectionDokument44 SeitenSampling sizeFull sampling of all patients with suspected thrombophlebitisand catheter associated blood stream infectionNandakishore RajkumarNoch keine Bewertungen
- Acute Nursing Care of The Older Adult With Fragility Hip Fracture An International Perspective Part 2 PDFDokument15 SeitenAcute Nursing Care of The Older Adult With Fragility Hip Fracture An International Perspective Part 2 PDFOktaNoch keine Bewertungen
- NCP - GeriaDokument4 SeitenNCP - GeriaMarielle J GarciaNoch keine Bewertungen
- PBL OsteomyelitisDokument27 SeitenPBL OsteomyelitisNabilah SufianNoch keine Bewertungen
- Complications of Bed Rest 1Dokument4 SeitenComplications of Bed Rest 1Geetha Bhavani100% (1)
- 08 Preventing In-Facility Pressure Ulcers As A Patient Safety StrategyDokument10 Seiten08 Preventing In-Facility Pressure Ulcers As A Patient Safety StrategyAmanda DavisNoch keine Bewertungen
- A Prospective Study of The Pressure Ulcer Scale For Healing (PUSH)Dokument5 SeitenA Prospective Study of The Pressure Ulcer Scale For Healing (PUSH)Sudhir MishraNoch keine Bewertungen
- Therapy Advice Following Below Knee AmputationDokument13 SeitenTherapy Advice Following Below Knee AmputationCatrinel ȘupialăNoch keine Bewertungen
- ULCER TREATMENTDokument83 SeitenULCER TREATMENTAashmi ChandrikaaNoch keine Bewertungen
- Anatomy and Physiology Lesson 2Dokument9 SeitenAnatomy and Physiology Lesson 2Kimberly Abellar LatoNoch keine Bewertungen
- SAB Empowering People With A Disability (ID 97381)Dokument70 SeitenSAB Empowering People With A Disability (ID 97381)amir abbasi0% (1)
- ColchonesDokument2 SeitenColchonesMMNoch keine Bewertungen
- WCET 2018 Programme Highlights Stomal Therapy, IncontinenceDokument36 SeitenWCET 2018 Programme Highlights Stomal Therapy, Incontinencesunandar fatwaNoch keine Bewertungen
- Pressure Ulcers: Problems and ChallengesDokument23 SeitenPressure Ulcers: Problems and Challengesedi edong100% (1)
- Back CareDokument17 SeitenBack CareHimani Patel100% (1)
- Jurnal Dekubitus Dengan Minyak KelapaDokument8 SeitenJurnal Dekubitus Dengan Minyak KelapaRatna SuminarNoch keine Bewertungen
- Jurnal Efektifitas Matras DekubitusDokument9 SeitenJurnal Efektifitas Matras DekubitusIhsan Nur MahmudiNoch keine Bewertungen
- C489 Task1 CompletedDokument4 SeitenC489 Task1 CompletedSteven SteveNoch keine Bewertungen