Das könnte Ihnen auch gefallen
- Tata AIG Health Insurance PDFDokument4 SeitenTata AIG Health Insurance PDFSrijan Tiwari80% (5)
- HDHC Health Insurance PDFDokument5 SeitenHDHC Health Insurance PDFNAYAN MEHTA0% (1)
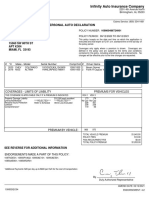
- Personal Auto Declaration: Infinity Auto Insurance CompanyDokument3 SeitenPersonal Auto Declaration: Infinity Auto Insurance CompanyDios Es AmorNoch keine Bewertungen
- Premium ReceiptDokument1 SeitePremium ReceiptVivekanand Gupta0% (2)
- Renewal ReceiptDokument1 SeiteRenewal ReceiptAnkit SinghNoch keine Bewertungen
- MediclaimDokument3 SeitenMediclaimPrajwal ShettyNoch keine Bewertungen
- Sasasasanisarisapa Mamathathathasanipapa Sasasasanisarisapa Mamathathathasanipapa Gamathanisa NirisaDokument2 SeitenSasasasanisarisapa Mamathathathasanipapa Sasasasanisarisapa Mamathathathasanipapa Gamathanisa NirisaLaxman RamesNoch keine Bewertungen
- CH 13Dokument16 SeitenCH 13April Lynn Horn33% (3)
- 2021 MDRT Mentoring PerformanceMonitoring Sheet TEMPLATEDokument6 Seiten2021 MDRT Mentoring PerformanceMonitoring Sheet TEMPLATEJanine KalaloNoch keine Bewertungen
- AXA Philippines FormDokument2 SeitenAXA Philippines FormRanieza CastilloNoch keine Bewertungen
- Axa Travel Claims Form Uae 1.1Dokument1 SeiteAxa Travel Claims Form Uae 1.1Baptiste ElliasNoch keine Bewertungen
- Investment Declaration Form - 2022-2023Dokument3 SeitenInvestment Declaration Form - 2022-2023Bharathi KNoch keine Bewertungen
- Certificate PDFDokument3 SeitenCertificate PDFSudeep MeshramNoch keine Bewertungen
- Construction Subcontractor Agreement: Page 1 of 8Dokument8 SeitenConstruction Subcontractor Agreement: Page 1 of 8Ronnie Jereza100% (1)
- Final Riverhead PBA Contract 2015-2020Dokument9 SeitenFinal Riverhead PBA Contract 2015-2020RiverheadLOCALNoch keine Bewertungen
- International Human Resource Case StudyDokument7 SeitenInternational Human Resource Case StudyAkua Serwaa AnsahNoch keine Bewertungen
- Proposer Details: Policy Details:: Quote Number: (4010/IP-00744175/000)Dokument3 SeitenProposer Details: Policy Details:: Quote Number: (4010/IP-00744175/000)Prakash WarrierNoch keine Bewertungen
- NNLA Credit Life OD Application Form 2022.04 FINALDokument2 SeitenNNLA Credit Life OD Application Form 2022.04 FINALBullet KanyembaNoch keine Bewertungen
- ABSLI Nishchit Aayush Plan - Policy Contract - V02Dokument28 SeitenABSLI Nishchit Aayush Plan - Policy Contract - V02Dattatraya Huvinahalli100% (1)
- Group Hospital and Surgical Claim FormDokument4 SeitenGroup Hospital and Surgical Claim FormYiki TanNoch keine Bewertungen
- Og 20 1000 9901 00271345Dokument6 SeitenOg 20 1000 9901 00271345Mukesh JangidNoch keine Bewertungen
- Report - 2023-03-23T141246.354Dokument3 SeitenReport - 2023-03-23T141246.354G Anil KumarNoch keine Bewertungen
- V Trans India Limited - WC Quote - PDFDokument3 SeitenV Trans India Limited - WC Quote - PDFVANAJAKSHI SNoch keine Bewertungen
- 4010ip-03083292001 QTDokument4 Seiten4010ip-03083292001 QTMayank SharmaNoch keine Bewertungen
- Manual PenjanaKerjaya 2.0Dokument2 SeitenManual PenjanaKerjaya 2.0Soo Ke XinNoch keine Bewertungen
- KMA Sacco Loan Application FormDokument4 SeitenKMA Sacco Loan Application FormDr. philemon mwongeraNoch keine Bewertungen
- Dated: 07/09/2022Dokument6 SeitenDated: 07/09/2022Fatin AsyuraNoch keine Bewertungen
- 2001 Isg Ren Opt1 12145 0Dokument13 Seiten2001 Isg Ren Opt1 12145 0Gobinath SekarNoch keine Bewertungen
- Proposal Form Group Personal Accident: Policy Details Nominee DetailsDokument1 SeiteProposal Form Group Personal Accident: Policy Details Nominee DetailsAbdul raheem syedNoch keine Bewertungen
- LVGI Policy ProposalDokument2 SeitenLVGI Policy Proposals KollaNoch keine Bewertungen
- GEMI Application Form - Two Wheeler LoansDokument5 SeitenGEMI Application Form - Two Wheeler LoansLuckyNoch keine Bewertungen
- Happy Family Floater-2015 Policy Schedule: UIN: IRDAI/HLT/OIC/P-H/V.II/450/15-16Dokument4 SeitenHappy Family Floater-2015 Policy Schedule: UIN: IRDAI/HLT/OIC/P-H/V.II/450/15-16Sanjay ShahNoch keine Bewertungen
- Reliance Covid-19 Indemnity Policy-Certificate of InsuranceDokument5 SeitenReliance Covid-19 Indemnity Policy-Certificate of InsurancePavan Kalyan UngaralaNoch keine Bewertungen
- Health Assurance UIN: IRDAI/HLT/MBHI/P-H/V.II/175/2016-17Dokument34 SeitenHealth Assurance UIN: IRDAI/HLT/MBHI/P-H/V.II/175/2016-17Sai Kiran ChandrasekharuniNoch keine Bewertungen
- Group Medicare Certificate of InsuranceDokument12 SeitenGroup Medicare Certificate of InsuranceMallikarjunayya HiremathNoch keine Bewertungen
- DuplicateDokument24 SeitenDuplicateanil.rohilla34Noch keine Bewertungen
- Oriental Insurance Company Health Policy DetailsDokument3 SeitenOriental Insurance Company Health Policy Detailsraja_tanukuNoch keine Bewertungen
- Marine Cargo - Open PolicyDokument3 SeitenMarine Cargo - Open PolicyMonti DabasNoch keine Bewertungen
- ICICI GMC Quote - Baroda Decorators Revised 02.04.2024Dokument6 SeitenICICI GMC Quote - Baroda Decorators Revised 02.04.2024silvershield.generalNoch keine Bewertungen
- Individual and Family Application Checklist (Uae) : How To ApplyDokument9 SeitenIndividual and Family Application Checklist (Uae) : How To ApplyJacob PriyadharshanNoch keine Bewertungen
- Non Death Claim FormDokument6 SeitenNon Death Claim FormHihiNoch keine Bewertungen
- Insurance Contract: Basic - Assurtous - Sante Health Insurance PolicyDokument4 SeitenInsurance Contract: Basic - Assurtous - Sante Health Insurance PolicySaratouNoch keine Bewertungen
- f54d2f7e-676b-48e0-8d7e-91f35d6f7f67Dokument77 Seitenf54d2f7e-676b-48e0-8d7e-91f35d6f7f67vasavi kNoch keine Bewertungen
- 0287764082 (1)Dokument8 Seiten0287764082 (1)rmohanNoch keine Bewertungen
- Premier Proposal 5f2bd12e92Dokument5 SeitenPremier Proposal 5f2bd12e92bajaj enterprisesNoch keine Bewertungen
- Agent Name: Indusind Bank Limited Agency Code: 004587369: 1.part ADokument39 SeitenAgent Name: Indusind Bank Limited Agency Code: 004587369: 1.part ANiraj DerkarNoch keine Bewertungen
- Proposal Form ScheduleDokument3 SeitenProposal Form ScheduleIndra MishraNoch keine Bewertungen
- Saudi EnayaDokument1 SeiteSaudi EnayaKareem EidNoch keine Bewertungen
- IRDA Registration No. 133 CIN No: U66010MH2006PLC165288: Part A Forwarding LetterDokument27 SeitenIRDA Registration No. 133 CIN No: U66010MH2006PLC165288: Part A Forwarding LetterChandan KeshriNoch keine Bewertungen
- Screenshot 20240131-145706 ChromeDokument2 SeitenScreenshot 20240131-145706 ChromeNagaraj VukkadapuNoch keine Bewertungen
- Insurance Form PDFDokument2 SeitenInsurance Form PDFSyed Tanveer Hasan HasanNoch keine Bewertungen
- ClaimFormDokument9 SeitenClaimFormVirat Vipul ChaudharyNoch keine Bewertungen
- Consolidated Policy ScheduleDokument3 SeitenConsolidated Policy Schedulepramod pawarNoch keine Bewertungen
- Acknowledgement Receipt - 20190331 - 205351Dokument1 SeiteAcknowledgement Receipt - 20190331 - 205351jay-ar barangay100% (1)
- Tone Wow Lindung - T&C - EngDokument6 SeitenTone Wow Lindung - T&C - EngAkmal HelmiNoch keine Bewertungen
- TW LINDUNG TNC - LATEST - 14122022 PDFDokument13 SeitenTW LINDUNG TNC - LATEST - 14122022 PDFluqman zuhariNoch keine Bewertungen
- Tata AigDokument3 SeitenTata AigAshik IkbalNoch keine Bewertungen
- Insurance CoverageDokument50 SeitenInsurance Coverage7dwg75s8mgNoch keine Bewertungen
- 48 2018 8424 PDFDokument4 Seiten48 2018 8424 PDFpushpa children hospitalNoch keine Bewertungen
- Life Planners Name: Arun Vasukula Life Planners Code: 004717547Dokument31 SeitenLife Planners Name: Arun Vasukula Life Planners Code: 004717547Vignesh BharathiNoch keine Bewertungen
- 29-08-2023 - Registrar Cir - Insurance Details - 443576221 - 1Dokument3 Seiten29-08-2023 - Registrar Cir - Insurance Details - 443576221 - 1GALLA SSHNoch keine Bewertungen
- Covid Indemnity Policy ScheduleDokument5 SeitenCovid Indemnity Policy ScheduleMerin LNoch keine Bewertungen
- Sudhir Kumar Jain Claim DocumentDokument10 SeitenSudhir Kumar Jain Claim Documentatul jaiswalNoch keine Bewertungen
- Ericson Insurance Tpa Pvt. Limited.: Cashless Authorization Letter (Part-D)Dokument3 SeitenEricson Insurance Tpa Pvt. Limited.: Cashless Authorization Letter (Part-D)baladon 007Noch keine Bewertungen
- Understanding Named, Automatic and Additional Insureds in the CGL PolicyVon EverandUnderstanding Named, Automatic and Additional Insureds in the CGL PolicyNoch keine Bewertungen
- NewtonChemF5 2.5 C-AcidsDokument11 SeitenNewtonChemF5 2.5 C-AcidsLaxman RamesNoch keine Bewertungen
- 13 1-HomeostasisDokument18 Seiten13 1-HomeostasisLaxman RamesNoch keine Bewertungen
- BIO EXP REPORT 16.3.3 Put&laxDokument4 SeitenBIO EXP REPORT 16.3.3 Put&laxLaxman RamesNoch keine Bewertungen
- Kingdom: Plantae Phylum: Tracheophyta Class: Magnoliopsida Order: Rafflesiales Family: Rafflesiaceae Genus: Rafflesia Species: Rafflesia ArnoldiiDokument3 SeitenKingdom: Plantae Phylum: Tracheophyta Class: Magnoliopsida Order: Rafflesiales Family: Rafflesiaceae Genus: Rafflesia Species: Rafflesia ArnoldiiLaxman RamesNoch keine Bewertungen
- Ifrs 17 Reinsurance Contract Held ExampleDokument24 SeitenIfrs 17 Reinsurance Contract Held ExampleHesham AlabaniNoch keine Bewertungen
- Axa Mansard Health Corporate Proposal Form: Dependents DetailsDokument1 SeiteAxa Mansard Health Corporate Proposal Form: Dependents DetailsGolden StarNoch keine Bewertungen
- Grocery Outlet Inc: 802920 Vendor: 48427 Ship To: 95 4/04/19Dokument3 SeitenGrocery Outlet Inc: 802920 Vendor: 48427 Ship To: 95 4/04/19Adrian UlloaNoch keine Bewertungen
- Directors and Officers LiabilityDokument2 SeitenDirectors and Officers LiabilityAyanda MabuthoNoch keine Bewertungen
- EFSA Guidelines On Outsourcing Requirements For Supervised EntitiesDokument17 SeitenEFSA Guidelines On Outsourcing Requirements For Supervised EntitiesarvoboxNoch keine Bewertungen
- Financial Planning Vs ForecastingDokument12 SeitenFinancial Planning Vs ForecastingKhiezna PakamNoch keine Bewertungen
- Straight Bill of LadingDokument2 SeitenStraight Bill of LadingHafizUmarArshad100% (1)
- Jim Powell Protectionist ParadiseDokument11 SeitenJim Powell Protectionist ParadiseGeorgeNoch keine Bewertungen
- Insurance PolicyDokument13 SeitenInsurance PolicyMeAnn TumbagaNoch keine Bewertungen
- LL.M. PART II (Semester III&IV)Dokument25 SeitenLL.M. PART II (Semester III&IV)mehakNoch keine Bewertungen
- Dosca Additional ManualDokument15 SeitenDosca Additional ManualFenziNoch keine Bewertungen
- MLZs ProjectDokument12 SeitenMLZs Projectkushagra khatriNoch keine Bewertungen
- TRADITIONAL LIFE MOCK EXAM - 03102015 v.1 PDFDokument8 SeitenTRADITIONAL LIFE MOCK EXAM - 03102015 v.1 PDFfrancisNoch keine Bewertungen
- San Miguel Brewery v. Law Union and Rock Insurance Co.Dokument1 SeiteSan Miguel Brewery v. Law Union and Rock Insurance Co.mackNoch keine Bewertungen
- Expression 21212Dokument26 SeitenExpression 21212Sharath VaddiparthiNoch keine Bewertungen
- Crisis and Incident ManagementDokument58 SeitenCrisis and Incident ManagementBlas de LezoNoch keine Bewertungen
- Usha Deep Academy of InsuranceDokument2 SeitenUsha Deep Academy of InsuranceRanjit SharmaNoch keine Bewertungen
- Glove Box GuideDokument2 SeitenGlove Box Guideevil_ironmindNoch keine Bewertungen
- Auto Insurance Quotes For Young DriversDokument10 SeitenAuto Insurance Quotes For Young DriversScott HoltNoch keine Bewertungen
- Present Value /future Value of Lumpsum/annuity InputsDokument4 SeitenPresent Value /future Value of Lumpsum/annuity InputsAshutosh BiswalNoch keine Bewertungen
- 11579Dokument4 Seiten11579api-309082881Noch keine Bewertungen
- Asha Insurance CompanyDokument38 SeitenAsha Insurance CompanyKamrul Hasan ShaonNoch keine Bewertungen
- Offer Cum Appointment Letter - C0252366Dokument16 SeitenOffer Cum Appointment Letter - C0252366mehravaibhav54Noch keine Bewertungen
- What To Bring WellsfargoDokument2 SeitenWhat To Bring WellsfargobrotherunkownNoch keine Bewertungen