Das könnte Ihnen auch gefallen
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (344)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (121)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (74)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- Character QuestionsDokument3 SeitenCharacter QuestionsAaron FarmerNoch keine Bewertungen
- Factors Associated With 30-Day Readmission For Patients Hospitalized For SeizuresDokument10 SeitenFactors Associated With 30-Day Readmission For Patients Hospitalized For SeizuresAndhika DNoch keine Bewertungen
- The Clinical Implications of Adult-Onset Henoch-Schonelin PurpuraDokument7 SeitenThe Clinical Implications of Adult-Onset Henoch-Schonelin PurpuraAndhika DNoch keine Bewertungen
- Attention Disorders in Adults With Epilepsy. Determinants and Therapeutic StrategiesDokument6 SeitenAttention Disorders in Adults With Epilepsy. Determinants and Therapeutic StrategiesAndhika DNoch keine Bewertungen
- Riginal Tudy: Sexually Transmitted Diseases Volume 43, Number 10, October 2016Dokument9 SeitenRiginal Tudy: Sexually Transmitted Diseases Volume 43, Number 10, October 2016Andhika DNoch keine Bewertungen
- Heart Failure in Adult Congenital Heart Disease Nonpharmacologic Treatment StrategiesDokument10 SeitenHeart Failure in Adult Congenital Heart Disease Nonpharmacologic Treatment StrategiesAndhika DNoch keine Bewertungen
- Chest: Passive Smoking Exposure Is Associated With Increased Risk of COPD in Never SmokersDokument7 SeitenChest: Passive Smoking Exposure Is Associated With Increased Risk of COPD in Never SmokersAndhika DNoch keine Bewertungen
- Risk Factors For Hypertension Among Young Adults (18-35) YearsDokument8 SeitenRisk Factors For Hypertension Among Young Adults (18-35) YearsAndhika DNoch keine Bewertungen
- Prevalence of Depression Symptoms in US Adults Before and During The COVID-19 PandemicDokument12 SeitenPrevalence of Depression Symptoms in US Adults Before and During The COVID-19 PandemicAndhika DNoch keine Bewertungen
- Effects of COVID-19 On College Students' Mental Health in The United States: Interview Survey StudyDokument14 SeitenEffects of COVID-19 On College Students' Mental Health in The United States: Interview Survey StudyAndhika DNoch keine Bewertungen
- The Prevalence and Risk Factors of Type 2 Diabetes Mellitus (DMT2) in A Semi-Urban Saudi PopulationDokument8 SeitenThe Prevalence and Risk Factors of Type 2 Diabetes Mellitus (DMT2) in A Semi-Urban Saudi PopulationAndhika DNoch keine Bewertungen
- Preview 2Dokument1 SeitePreview 2Andhika DNoch keine Bewertungen
- (Type The Documen T Title) : (Year)Dokument18 Seiten(Type The Documen T Title) : (Year)goodluck788Noch keine Bewertungen
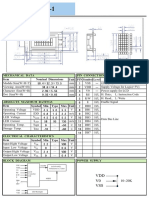
- V0 VSS VDD: Unit PIN Symbol Level Nominal Dimensions Pin Connections Function Mechanical Data ItemDokument1 SeiteV0 VSS VDD: Unit PIN Symbol Level Nominal Dimensions Pin Connections Function Mechanical Data ItemBasir Ahmad NooriNoch keine Bewertungen
- Intermolecular Force Worksheet KeyDokument3 SeitenIntermolecular Force Worksheet KeyBill alfonsoNoch keine Bewertungen
- NCERT Exemplar Class 7 Maths IntegersDokument661 SeitenNCERT Exemplar Class 7 Maths IntegersRohiniNoch keine Bewertungen
- One Page Mistake ProofingDokument1 SeiteOne Page Mistake Proofingtuan mai vanNoch keine Bewertungen
- Creativity MCQDokument17 SeitenCreativity MCQAmanVatsNoch keine Bewertungen
- 10 AI Summer Vacation HWDokument2 Seiten10 AI Summer Vacation HWAyushi SinghNoch keine Bewertungen
- EER Model: Enhance Entity Relationship ModelDokument12 SeitenEER Model: Enhance Entity Relationship ModelHaroon KhalidNoch keine Bewertungen
- Basic Task 315Dokument9 SeitenBasic Task 315gaikwadamitag1Noch keine Bewertungen
- Proper Storage of Instruments2Dokument20 SeitenProper Storage of Instruments2Pierre Vincent PorrasNoch keine Bewertungen
- Principal's Corner: School ProfileDokument7 SeitenPrincipal's Corner: School ProfileAngel Mae LabadorNoch keine Bewertungen
- Current Office Phone Number Vijayawada, Andhra Pradesh (A.p.)Dokument11 SeitenCurrent Office Phone Number Vijayawada, Andhra Pradesh (A.p.)Manoj Digi Loans100% (1)
- Lac CultureDokument7 SeitenLac CultureDhruboNoch keine Bewertungen
- ASN PyariViswamResumeDokument3 SeitenASN PyariViswamResumeapi-27019513100% (2)
- What Is Situational Coaching and When To Use ItDokument3 SeitenWhat Is Situational Coaching and When To Use ItBrian KamoedNoch keine Bewertungen
- Refrigeration and Air ConditioningDokument41 SeitenRefrigeration and Air Conditioningrejeesh_rajendranNoch keine Bewertungen
- Sharding:: Vertical Scaling Involves Increasing The Capacity of A Single Server, Such As Using A More Powerful CPUDokument233 SeitenSharding:: Vertical Scaling Involves Increasing The Capacity of A Single Server, Such As Using A More Powerful CPUJigar SutariyaNoch keine Bewertungen
- 3.Space-Activity BookDokument21 Seiten3.Space-Activity BookRania FarranNoch keine Bewertungen
- MAS500 2011 Vår Masteroppgave Henrik Engedal Per Magne EgelidDokument130 SeitenMAS500 2011 Vår Masteroppgave Henrik Engedal Per Magne EgelidPoppy DanielsNoch keine Bewertungen
- Good Parenting 1Dokument6 SeitenGood Parenting 1honey13Noch keine Bewertungen
- Chapter 1 To7 With Course OutlineDokument34 SeitenChapter 1 To7 With Course Outlinerk_kamatchi3483Noch keine Bewertungen
- 09-Hispec DespecDokument51 Seiten09-Hispec DespecHyungon KimNoch keine Bewertungen
- Air Washer Test RigDokument5 SeitenAir Washer Test RigJagdish Singh MehtaNoch keine Bewertungen
- ABC Press Release and AllocationDokument28 SeitenABC Press Release and AllocationAndrew Finn KlauberNoch keine Bewertungen
- Toro 006Dokument2 SeitenToro 006Eric CNoch keine Bewertungen
- Action Research MethodDokument27 SeitenAction Research MethodNiño Czar RaroNoch keine Bewertungen
- BONENT Candidate Handbook PDFDokument28 SeitenBONENT Candidate Handbook PDFParshanwa Johnson100% (1)
- What Is A RubricDokument2 SeitenWhat Is A Rubricjasmina2869Noch keine Bewertungen
- Preparation of Giemsa Working SolutionDokument4 SeitenPreparation of Giemsa Working SolutionMUHAMMAD DIMAS YUSUF 1903031Noch keine Bewertungen