Das könnte Ihnen auch gefallen
- 9fetal Well Being in PregnancyDokument10 Seiten9fetal Well Being in PregnancyuouoNoch keine Bewertungen
- Thyroid Disease in PregnancyDokument36 SeitenThyroid Disease in Pregnancypeni_dwiNoch keine Bewertungen
- Principles and Interpretation of CardiotocographyDokument9 SeitenPrinciples and Interpretation of CardiotocographyCKNoch keine Bewertungen
- Shock and HemorrhageDokument29 SeitenShock and HemorrhageDr djNoch keine Bewertungen
- CRF in PregnancyDokument27 SeitenCRF in PregnancyJitendra AgrawalNoch keine Bewertungen
- The Concept of ManagementDokument3 SeitenThe Concept of ManagementViresh YadavNoch keine Bewertungen
- Maternal Satisfaction On Nursing Care Among Postnatal Mothers in Selected Teaching Hospital, Kaski DistrictDokument6 SeitenMaternal Satisfaction On Nursing Care Among Postnatal Mothers in Selected Teaching Hospital, Kaski DistrictInternational Journal of Innovative Science and Research TechnologyNoch keine Bewertungen
- Twenty Point Programme by Varnit VashisthaDokument9 SeitenTwenty Point Programme by Varnit VashisthaVarnit VashishtaNoch keine Bewertungen
- Menstrual Hygiene: School Health ProgramDokument18 SeitenMenstrual Hygiene: School Health ProgramDeekshya DevkotaNoch keine Bewertungen
- Journal Homepage: - : IntroductionDokument4 SeitenJournal Homepage: - : IntroductionIJAR JOURNALNoch keine Bewertungen
- Biophysical AssessmentDokument9 SeitenBiophysical AssessmentSanjeev NambalateNoch keine Bewertungen
- Advanced Nursing PracticeDokument8 SeitenAdvanced Nursing PracticePrasanna KumarNoch keine Bewertungen
- Imaging in PregnancyDokument8 SeitenImaging in PregnancyKeeranmayeeishraNoch keine Bewertungen
- Growth - Development of Fetus - NeonateDokument40 SeitenGrowth - Development of Fetus - NeonatesujidahNoch keine Bewertungen
- Infertility 230411173332 Cc62ed95Dokument50 SeitenInfertility 230411173332 Cc62ed95Kapil YadavNoch keine Bewertungen
- Presentation FPAI 2014 2Dokument20 SeitenPresentation FPAI 2014 2Sameer Dubey0% (1)
- Women &mental HealthDokument16 SeitenWomen &mental HealthDhAiRyA ArOrANoch keine Bewertungen
- Infertilityseminarppt 190718134710Dokument77 SeitenInfertilityseminarppt 190718134710subiNoch keine Bewertungen
- Ministry of Health and Family Welfare Pregnancy GuidelinesDokument173 SeitenMinistry of Health and Family Welfare Pregnancy GuidelinesKhushi GuptaNoch keine Bewertungen
- Effect of A Training Program About Maternal Fetal Attachment Skills On Prenatal Attachment Among Primigravida WomenDokument6 SeitenEffect of A Training Program About Maternal Fetal Attachment Skills On Prenatal Attachment Among Primigravida WomenInternational Organization of Scientific Research (IOSR)Noch keine Bewertungen
- Menstrual Disorders and Menstrual Hygiene PracticesDokument5 SeitenMenstrual Disorders and Menstrual Hygiene PracticesChikita Artia SariNoch keine Bewertungen
- Prevention of Parent To Child Transmission of HIV : Dr. ShobhaDokument52 SeitenPrevention of Parent To Child Transmission of HIV : Dr. ShobhajijaniNoch keine Bewertungen
- 2017 STP Paed Neonates PDFDokument258 Seiten2017 STP Paed Neonates PDFChoden JamyangNoch keine Bewertungen
- Family Planning Methods - LatestDokument59 SeitenFamily Planning Methods - LatestGenevieve VillaflorNoch keine Bewertungen
- Diagnosi S: MalariaDokument28 SeitenDiagnosi S: MalariaOm Prakash SinghNoch keine Bewertungen
- External ExaminationDokument16 SeitenExternal Examinationrejoice international100% (1)
- Formulation of NCPDokument8 SeitenFormulation of NCPSandeep choudharyNoch keine Bewertungen
- PromotionDokument22 SeitenPromotioncpadiyarNoch keine Bewertungen
- HysterectomyDokument5 SeitenHysterectomysapana shah100% (1)
- Orems Self Care Deficit Nursing TheoryDokument30 SeitenOrems Self Care Deficit Nursing TheoryAra Jean AgapitoNoch keine Bewertungen
- Diabetes in PregnancyDokument11 SeitenDiabetes in PregnancyAlana CaballeroNoch keine Bewertungen
- Hyper Bilirubin Emi ADokument29 SeitenHyper Bilirubin Emi ANinz NunezNoch keine Bewertungen
- Pregnancy Thyroid Disease 508Dokument12 SeitenPregnancy Thyroid Disease 508Ankush RanaNoch keine Bewertungen
- Pap Smear - Overview, Indications, PreparationDokument11 SeitenPap Smear - Overview, Indications, PreparationBayu Surya DanaNoch keine Bewertungen
- Grupo 10 Non-Technical Skills in HistopathologyDokument9 SeitenGrupo 10 Non-Technical Skills in HistopathologySantos Pardo Gomez100% (1)
- IUCD Manual EnglishDokument194 SeitenIUCD Manual EnglishHarshaWakodkarNoch keine Bewertungen
- Prevalence of Anemia Among Adolescent GirlsDokument6 SeitenPrevalence of Anemia Among Adolescent GirlsYolanda SimamoraNoch keine Bewertungen
- Importance of Research in NursingDokument5 SeitenImportance of Research in NursingAleena ShibuNoch keine Bewertungen
- Mission, Vision, Philosophy and ObjectivesDokument49 SeitenMission, Vision, Philosophy and ObjectivesNeethu JoseNoch keine Bewertungen
- Induction of LabourDokument51 SeitenInduction of LabourSarita PariyarNoch keine Bewertungen
- Who Labour Care GuideDokument1 SeiteWho Labour Care Guidezeus balagtasNoch keine Bewertungen
- Menstrual CycleDokument19 SeitenMenstrual Cycleraghuram reddyNoch keine Bewertungen
- Bunt - Male and Female Infertility USAFP 2009-v2 (PPTminimizer)Dokument35 SeitenBunt - Male and Female Infertility USAFP 2009-v2 (PPTminimizer)Jalajarani AridassNoch keine Bewertungen
- Psy - Nursing Care Plan - Therapeutic CommunicationDokument6 SeitenPsy - Nursing Care Plan - Therapeutic CommunicationCarmen Angela DusaranNoch keine Bewertungen
- Abortion India Lit ReviewDokument48 SeitenAbortion India Lit ReviewPrathibha GuruguriNoch keine Bewertungen
- InfertilityDokument29 SeitenInfertilityCristina StanleeNoch keine Bewertungen
- S36Dokument13 SeitenS36Srusti PatelNoch keine Bewertungen
- Efficacy of Planned Education Programme On Knowledge Related To Hormonal Replacement Therapy Among Menopausal Women at Selected Rural Areas in MysuruDokument6 SeitenEfficacy of Planned Education Programme On Knowledge Related To Hormonal Replacement Therapy Among Menopausal Women at Selected Rural Areas in MysuruInternational Journal of Innovative Science and Research TechnologyNoch keine Bewertungen
- Lesson Plan of Conference PDFDokument44 SeitenLesson Plan of Conference PDFRahul DamorNoch keine Bewertungen
- Rights of Special GroupsDokument33 SeitenRights of Special GroupsbellaNoch keine Bewertungen
- Category Health Workers PDFDokument37 SeitenCategory Health Workers PDFAparna Kingini100% (1)
- Hiv in PregnancyDokument98 SeitenHiv in PregnancyAkrit DahalNoch keine Bewertungen
- Major Stake Holders in Health Care System-GovernmentDokument22 SeitenMajor Stake Holders in Health Care System-GovernmentTanviNoch keine Bewertungen
- 1040 Inventory Control Condemnation ProceduresDokument44 Seiten1040 Inventory Control Condemnation ProceduresnagssaraNoch keine Bewertungen
- KULDEEP Synopsis Mad by MeDokument18 SeitenKULDEEP Synopsis Mad by MeKuldeep SharmaNoch keine Bewertungen
- Genetic CounsellingDokument12 SeitenGenetic CounsellingPATEL NEHAKUMARI VIMALBHAINoch keine Bewertungen
- Lobbying: Prepared by Binju Karki M.SC - NursingDokument26 SeitenLobbying: Prepared by Binju Karki M.SC - NursingBhawna JoshiNoch keine Bewertungen
- Immunization Programme: National Health MissionDokument11 SeitenImmunization Programme: National Health MissionAnimaNoch keine Bewertungen
- D) Signs and Symptoms of Pregnancy (Ed)Dokument9 SeitenD) Signs and Symptoms of Pregnancy (Ed)Trina Joy DomantayNoch keine Bewertungen
- Handbook of Current and Novel Protocols for the Treatment of InfertilityVon EverandHandbook of Current and Novel Protocols for the Treatment of InfertilityMichael H. DahanNoch keine Bewertungen
- Anemia in Pregnancy B.JDokument39 SeitenAnemia in Pregnancy B.JBhawna JoshiNoch keine Bewertungen
- School of Nursing Science and Research, Sharda UniversityDokument12 SeitenSchool of Nursing Science and Research, Sharda UniversityBhawna JoshiNoch keine Bewertungen
- 1 WichamDokument34 Seiten1 WichamBhawna JoshiNoch keine Bewertungen
- StomachGastricCancerDokument12 SeitenStomachGastricCancerBhawna JoshiNoch keine Bewertungen
- 1 2019007280 Samjhana Neupane Community Health Nursing Pro. Sreeraja Kumar (Dean, SNSR)Dokument3 Seiten1 2019007280 Samjhana Neupane Community Health Nursing Pro. Sreeraja Kumar (Dean, SNSR)Bhawna JoshiNoch keine Bewertungen
- School of Nursing Science and Research Sharda UniversityDokument5 SeitenSchool of Nursing Science and Research Sharda UniversityBhawna JoshiNoch keine Bewertungen
- Attendance July MonthDokument22 SeitenAttendance July MonthBhawna JoshiNoch keine Bewertungen
- School of Nursing Science and ResearchDokument38 SeitenSchool of Nursing Science and ResearchBhawna JoshiNoch keine Bewertungen
- School of Nursing Science and Research, Sharda UniversityDokument15 SeitenSchool of Nursing Science and Research, Sharda UniversityBhawna Joshi100% (1)
- S.N. System ID Name Speciality Guide: School of Nursing and ResearchDokument6 SeitenS.N. System ID Name Speciality Guide: School of Nursing and ResearchBhawna JoshiNoch keine Bewertungen
- Overview of Research ProcessDokument6 SeitenOverview of Research ProcessBhawna JoshiNoch keine Bewertungen
- 1st International ConferenceDokument6 Seiten1st International ConferenceBhawna JoshiNoch keine Bewertungen
- Sharda Synopsis Presentation J.KDokument9 SeitenSharda Synopsis Presentation J.KBhawna JoshiNoch keine Bewertungen
- Quiz On ANPDokument9 SeitenQuiz On ANPBhawna JoshiNoch keine Bewertungen
- Full Report New Registration Details:: Applicant Name: Applicant Number: DobDokument2 SeitenFull Report New Registration Details:: Applicant Name: Applicant Number: DobBhawna JoshiNoch keine Bewertungen
- Professional Education: PREPARED By-Shilpy MittaDokument30 SeitenProfessional Education: PREPARED By-Shilpy MittaBhawna JoshiNoch keine Bewertungen
- Procedure On Abdominal ParacentsisDokument22 SeitenProcedure On Abdominal ParacentsisBhawna JoshiNoch keine Bewertungen
- School of Nursing Science and Research, Sharda University, Greater NoidaDokument6 SeitenSchool of Nursing Science and Research, Sharda University, Greater NoidaBhawna JoshiNoch keine Bewertungen
- Nightingale Institute of Nursing Noida: ON A.V. Aids Exhibition (Subject - Nursing Education)Dokument6 SeitenNightingale Institute of Nursing Noida: ON A.V. Aids Exhibition (Subject - Nursing Education)Bhawna JoshiNoch keine Bewertungen
- Over View of Research ProcessDokument27 SeitenOver View of Research ProcessBhawna JoshiNoch keine Bewertungen
- 1a 1Dokument21 Seiten1a 1Bhawna JoshiNoch keine Bewertungen
- Abstra CT: DAT ADokument35 SeitenAbstra CT: DAT ABhawna JoshiNoch keine Bewertungen
- Company Law II ProjectDokument21 SeitenCompany Law II ProjectBhawna JoshiNoch keine Bewertungen
- 1a 1Dokument21 Seiten1a 1Bhawna JoshiNoch keine Bewertungen
- Historical Evolution of Nursing ResearchDokument28 SeitenHistorical Evolution of Nursing ResearchBhawna Joshi86% (7)
- NSG Education Quiz 24 June 2020Dokument2 SeitenNSG Education Quiz 24 June 2020Bhawna JoshiNoch keine Bewertungen
- Chapter 3Dokument6 SeitenChapter 3MoiMoi P.S.Noch keine Bewertungen
- Swyer SyndromeDokument1 SeiteSwyer SyndromeHaNoch keine Bewertungen
- MCHN Reproductive SystemDokument3 SeitenMCHN Reproductive SystemShaira PacallesNoch keine Bewertungen
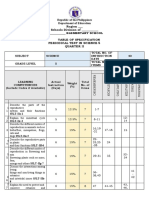
- Periodical Test in Science5 q2Dokument8 SeitenPeriodical Test in Science5 q2FMP Music0% (1)
- Flash On: English For NursingDokument16 SeitenFlash On: English For NursingNarcisaNoch keine Bewertungen
- People vs. CampuhanDokument7 SeitenPeople vs. CampuhanMJ BautistaNoch keine Bewertungen
- Anatomi Dasar 2Dokument19 SeitenAnatomi Dasar 2Dwi Ananda GunawanNoch keine Bewertungen
- Sex-Change Chicken Gertie The Hen Becomes Bertie The CockerelDokument2 SeitenSex-Change Chicken Gertie The Hen Becomes Bertie The Cockereldraco amiceNoch keine Bewertungen
- Anatomy PhysiologyDokument3 SeitenAnatomy PhysiologyRouie Björn ABrianNoch keine Bewertungen
- Menstrual Cycle PhasesDokument2 SeitenMenstrual Cycle PhasesPatricia G ChiuNoch keine Bewertungen
- Physical Development in AdolescenceDokument30 SeitenPhysical Development in AdolescenceKJ MarquezNoch keine Bewertungen
- Lab 10 Semen AnalysisDokument45 SeitenLab 10 Semen AnalysisFeroz KhanNoch keine Bewertungen
- Spermatogenesis 1Dokument28 SeitenSpermatogenesis 1LellllNoch keine Bewertungen
- Miracle of LifeDokument3 SeitenMiracle of Lifespankey0809Noch keine Bewertungen
- Ge Elec 2 - Gender and Society Reviewer - 015506Dokument6 SeitenGe Elec 2 - Gender and Society Reviewer - 015506Nonito ValeNoch keine Bewertungen
- Physiology of PregnancyDokument27 SeitenPhysiology of PregnancysabaNoch keine Bewertungen
- Gynae 64Dokument14 SeitenGynae 64Jha K SujitNoch keine Bewertungen
- Q1 &Q2 1st Summative Test Science 5 EDITEDDokument14 SeitenQ1 &Q2 1st Summative Test Science 5 EDITEDTrishaAnnSantiagoFidel100% (2)
- ThesisDokument5 SeitenThesisJulia ConceNoch keine Bewertungen
- Gynecomastia Incidence Causes and TreatmentDokument9 SeitenGynecomastia Incidence Causes and TreatmentAqshaNoch keine Bewertungen
- Congenital and Acquired Malformations in Vulva and Vagina - Pediatric AgeDokument2 SeitenCongenital and Acquired Malformations in Vulva and Vagina - Pediatric AgePramedicaPerdanaPutraNoch keine Bewertungen
- Vagina - Google SearchDokument1 SeiteVagina - Google SearchAbdullah AlthobaitiNoch keine Bewertungen
- Montfort Senior Secondary School: Sundaranadappu, SivagangaiDokument9 SeitenMontfort Senior Secondary School: Sundaranadappu, SivagangaiRoss GellerNoch keine Bewertungen
- Dr. Akash Vaidya PPT On AnoestrusDokument15 SeitenDr. Akash Vaidya PPT On AnoestrusAkash VaidyaNoch keine Bewertungen
- Learning Activity Sheet 3.1: Melc 1Dokument7 SeitenLearning Activity Sheet 3.1: Melc 1Ricah PrestonNoch keine Bewertungen
- Dev Psych Adolescence Unit 6Dokument28 SeitenDev Psych Adolescence Unit 6zaryabali771Noch keine Bewertungen
- Physical and Sexual Self - Lesson 1Dokument22 SeitenPhysical and Sexual Self - Lesson 1MICHELE ANGELA HEREBESINoch keine Bewertungen
- Week 2-3 Part 1Dokument26 SeitenWeek 2-3 Part 1EmpieNoch keine Bewertungen
- Assisted Reproductive Technology (ART) : and ApplicationDokument38 SeitenAssisted Reproductive Technology (ART) : and ApplicationPraluki HerliawanNoch keine Bewertungen
- Chapter 1 - UtsDokument5 SeitenChapter 1 - UtsJeng JengNoch keine Bewertungen