Das könnte Ihnen auch gefallen
- Average Waves in Unprotected Waters by Anne Tyler - Summary PDFDokument1 SeiteAverage Waves in Unprotected Waters by Anne Tyler - Summary PDFRK PADHI0% (1)
- Testicular Torsion, Peds Cases NotesDokument1 SeiteTesticular Torsion, Peds Cases NotesdzalhcNoch keine Bewertungen
- Spine & Extremities / Abdomen / Neurologic Exam: PalpationDokument8 SeitenSpine & Extremities / Abdomen / Neurologic Exam: PalpationBrent DizonNoch keine Bewertungen
- PD 3.2 Alterations in GI Function Part 1Dokument6 SeitenPD 3.2 Alterations in GI Function Part 1Kim DeeNoch keine Bewertungen
- Aortic Aneurysm-: NUR2744 Test 3 OutlineDokument10 SeitenAortic Aneurysm-: NUR2744 Test 3 Outlinemara5140Noch keine Bewertungen
- 2 Nutritional Metabolic PatternDokument22 Seiten2 Nutritional Metabolic PatternMyles Zen Dieta EaNoch keine Bewertungen
- Emergenze Addome RXDokument9 SeitenEmergenze Addome RXBrovazzo PieroNoch keine Bewertungen
- Health Assessment: AbdomenDokument18 SeitenHealth Assessment: AbdomenBatiao Camille ClaireNoch keine Bewertungen
- LEC 1 - Abdomen 1 2009 OLDDokument3 SeitenLEC 1 - Abdomen 1 2009 OLDElle ReyesNoch keine Bewertungen
- Vi. Nursing Care Plan Cues Analysis Nursing Diagnosis Goal / Plan Intervention Rationale EvaluationDokument2 SeitenVi. Nursing Care Plan Cues Analysis Nursing Diagnosis Goal / Plan Intervention Rationale EvaluationRaisa Robelle QuichoNoch keine Bewertungen
- Disorders of Lower Urinary TractDokument5 SeitenDisorders of Lower Urinary TractMuhammadR1Noch keine Bewertungen
- Abdominal HerniaDokument2 SeitenAbdominal HerniaAshan BopitiyaNoch keine Bewertungen
- (Pedia 3a) Neonat BDokument21 Seiten(Pedia 3a) Neonat BZai Ra DianaNoch keine Bewertungen
- (Surgery) Midterms PediatricsDokument5 Seiten(Surgery) Midterms Pediatricsalmira.s.mercadoNoch keine Bewertungen
- CORNELL NOTE Physical and Developmental Disorders in NewbornDokument4 SeitenCORNELL NOTE Physical and Developmental Disorders in NewbornMargareth DandanNoch keine Bewertungen
- 3 - Lower Gastrointestinal DisorderDokument14 Seiten3 - Lower Gastrointestinal DisorderNica EnriquezNoch keine Bewertungen
- Vermicular AppendixDokument3 SeitenVermicular AppendixMuhaimin AbdullahNoch keine Bewertungen
- French 16 - AppendixDokument5 SeitenFrench 16 - AppendixPrince VallejosNoch keine Bewertungen
- Physical ExamdocxDokument94 SeitenPhysical ExamdocxKalashini SenadheeraNoch keine Bewertungen
- Esophageal DiverticulaDokument13 SeitenEsophageal DiverticulaShekaira B. SimsimNoch keine Bewertungen
- 03 Abdominal TraumaDokument1 Seite03 Abdominal Traumabunso padillaNoch keine Bewertungen
- Review - Acute Care Surgery Part 1Dokument63 SeitenReview - Acute Care Surgery Part 1Loveknot BG BoripbinNoch keine Bewertungen
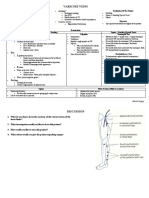
- Varicose Veins: Short History Positioning of The PatientDokument2 SeitenVaricose Veins: Short History Positioning of The PatientAshan BopitiyaNoch keine Bewertungen
- XXXDokument13 SeitenXXXtiaraNoch keine Bewertungen
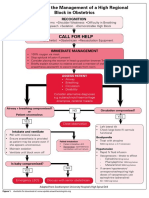
- Algorithm For The Management of A High Regional Block in ObstetricsDokument5 SeitenAlgorithm For The Management of A High Regional Block in ObstetricsRaditya DidotNoch keine Bewertungen
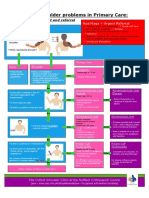
- Pathway For Shoulder PainDokument1 SeitePathway For Shoulder Painrizk86Noch keine Bewertungen
- Textbook of Paediatrics Part 1Dokument1 SeiteTextbook of Paediatrics Part 1Soz P. KawaniNoch keine Bewertungen
- Pediatric Gastrointestinal DisordersDokument11 SeitenPediatric Gastrointestinal DisordersANGELTHERESE CANDIANoch keine Bewertungen
- Lower GIT 1Dokument15 SeitenLower GIT 1Zuhra JabeenNoch keine Bewertungen
- Preceptorial Format 2023 Group 2Dokument5 SeitenPreceptorial Format 2023 Group 2Cayla DeniceNoch keine Bewertungen
- Abdominal TraumaDokument1 SeiteAbdominal TraumaYalc LapidNoch keine Bewertungen
- Abdominal AssessmentDokument7 SeitenAbdominal AssessmentGlen DaleNoch keine Bewertungen
- Gynecological Assessment: DateDokument4 SeitenGynecological Assessment: Dateanne laureNoch keine Bewertungen
- Pediatric Surg TransDokument4 SeitenPediatric Surg TransSven OrdanzaNoch keine Bewertungen
- 7 Abdominal TraumaDokument9 Seiten7 Abdominal TraumaMyrtle Yvonne RagubNoch keine Bewertungen
- NHS UK Diagnosis of Shoulder ProblemsDokument1 SeiteNHS UK Diagnosis of Shoulder ProblemsmertNoch keine Bewertungen
- Cardiovascular Examination IBDDokument6 SeitenCardiovascular Examination IBDTRINIDAD, ALYANNA V.Noch keine Bewertungen
- Acute Painful Scrotum: ALGORITHM-Suspicion For Testicular TorsionDokument13 SeitenAcute Painful Scrotum: ALGORITHM-Suspicion For Testicular TorsionM. ANDRI PRASETYONoch keine Bewertungen
- Subjetive: Long Term: Independent:: RationaleDokument1 SeiteSubjetive: Long Term: Independent:: RationaleRyann BuayaNoch keine Bewertungen
- 1 - Abdomen 1Dokument23 Seiten1 - Abdomen 1noushad aminNoch keine Bewertungen
- Holy Child School of Davao Nursing Care Plan: E. Jacinto St. Davao CityDokument2 SeitenHoly Child School of Davao Nursing Care Plan: E. Jacinto St. Davao CityMaxileo Villareal AbeciaNoch keine Bewertungen
- Nursing Care Plan Abrubtio PlacentaDokument2 SeitenNursing Care Plan Abrubtio PlacentaLei Ortega0% (1)
- Assessing AbdomenDokument33 SeitenAssessing Abdomenjaypee01Noch keine Bewertungen
- 116 - Alterations in GI EliminationDokument12 Seiten116 - Alterations in GI EliminationGino-o, KyleNoch keine Bewertungen
- Novilyn C. Pataray BSN - Ii: Assessment Diagnosi S Pathophysiology Planning Intervention Rationale EvaluationDokument1 SeiteNovilyn C. Pataray BSN - Ii: Assessment Diagnosi S Pathophysiology Planning Intervention Rationale EvaluationCharina Aubrey100% (1)
- NCPDokument2 SeitenNCPJoanne Pascual TuasonNoch keine Bewertungen
- Nursing Care Plan Ectopic PregnancyDokument2 SeitenNursing Care Plan Ectopic Pregnancyderic90% (39)
- NCP Case 6Dokument1 SeiteNCP Case 6Eduard GarchitorenaNoch keine Bewertungen
- Abdominal Assessment HA LectureDokument44 SeitenAbdominal Assessment HA LectureKatrina BeltranNoch keine Bewertungen
- 1.0 Achalasia & Pyloric StenosisDokument1 Seite1.0 Achalasia & Pyloric StenosisRaman kangNoch keine Bewertungen
- S T A R T: Imple Riage ND Apid ReatmentDokument17 SeitenS T A R T: Imple Riage ND Apid ReatmentNavine NavNoch keine Bewertungen
- Acute Low Back Pain Flowchart January 2017Dokument1 SeiteAcute Low Back Pain Flowchart January 20171234chocoNoch keine Bewertungen
- Special Test - Lecture Notes 1 Special Test - Lecture Notes 1Dokument18 SeitenSpecial Test - Lecture Notes 1 Special Test - Lecture Notes 1Anne SerneoNoch keine Bewertungen
- Learning Objectives For EXAM 1Dokument13 SeitenLearning Objectives For EXAM 1bcvaughn019Noch keine Bewertungen
- Abdominal PainDokument6 SeitenAbdominal PainHynne Jhea EchavezNoch keine Bewertungen
- Killings and Death of Conscience'Dokument1 SeiteKillings and Death of Conscience'Frances Isabella OlasimanNoch keine Bewertungen
- Metropolitan Waterworks and Sewerage SystemDokument1 SeiteMetropolitan Waterworks and Sewerage SystemFrances Isabella OlasimanNoch keine Bewertungen
- 5 Bleeding Disorders PPT EditedDokument87 Seiten5 Bleeding Disorders PPT EditedFrances Isabella OlasimanNoch keine Bewertungen
- No Oral HygieneDokument14 SeitenNo Oral HygieneFrances Isabella OlasimanNoch keine Bewertungen
- 1 - Principles of Plastic, Reconstructive and Aesthetic Surgery EDITEDDokument3 Seiten1 - Principles of Plastic, Reconstructive and Aesthetic Surgery EDITEDFrances Isabella OlasimanNoch keine Bewertungen
- Form No. 10-I: Certificate of Prescribed Authority For The Purposes of Section 80DDBDokument1 SeiteForm No. 10-I: Certificate of Prescribed Authority For The Purposes of Section 80DDBIam KarthikeyanNoch keine Bewertungen
- Easter in RomaniaDokument5 SeitenEaster in RomaniaDragos IonutNoch keine Bewertungen
- Comfrey Materia Medica HerbsDokument17 SeitenComfrey Materia Medica HerbsAlejandra Guerrero100% (1)
- Rubrics For Field Trip 1 Reflective DiaryDokument2 SeitenRubrics For Field Trip 1 Reflective DiarycrystalNoch keine Bewertungen
- Effect of Intensive Health Education On Adherence To Treatment in Sputum Positive Pulmonary Tuberculosis PatientsDokument6 SeitenEffect of Intensive Health Education On Adherence To Treatment in Sputum Positive Pulmonary Tuberculosis PatientspocutindahNoch keine Bewertungen
- Google Automatically Generates HTML Versions of Documents As We Crawl The WebDokument2 SeitenGoogle Automatically Generates HTML Versions of Documents As We Crawl The Websuchi ravaliaNoch keine Bewertungen
- Coronally Advanced Flap With Connective Tissue GraDokument13 SeitenCoronally Advanced Flap With Connective Tissue GrasutriNoch keine Bewertungen
- HIS Unit COMBINES Two Birthdays:: George Washington's BirthdayDokument9 SeitenHIS Unit COMBINES Two Birthdays:: George Washington's BirthdayOscar Panez LizargaNoch keine Bewertungen
- Capacitor Banks in Power System Part FourDokument4 SeitenCapacitor Banks in Power System Part FourTigrillo100% (1)
- F3 Eng Mid-Term 2023Dokument5 SeitenF3 Eng Mid-Term 2023Mwinyi BlogNoch keine Bewertungen
- Simple Past TenselDokument3 SeitenSimple Past TenselPutra ViskellaNoch keine Bewertungen
- Bgs Chapter 2Dokument33 SeitenBgs Chapter 2KiranShettyNoch keine Bewertungen
- Prime White Cement vs. Iac Assigned CaseDokument6 SeitenPrime White Cement vs. Iac Assigned CaseStephanie Reyes GoNoch keine Bewertungen
- Key Performance IndicatorsDokument15 SeitenKey Performance IndicatorsAbdul HafeezNoch keine Bewertungen
- Cruz-Arevalo v. Layosa DigestDokument2 SeitenCruz-Arevalo v. Layosa DigestPatricia Ann RueloNoch keine Bewertungen
- Pediatric Autonomic DisorderDokument15 SeitenPediatric Autonomic DisorderaimanNoch keine Bewertungen
- Sucesos de Las Islas Filipinas PPT Content - Carlos 1Dokument2 SeitenSucesos de Las Islas Filipinas PPT Content - Carlos 1A Mi YaNoch keine Bewertungen
- Hygiene and HealthDokument2 SeitenHygiene and HealthMoodaw SoeNoch keine Bewertungen
- Birds (Aves) Are A Group Of: WingsDokument1 SeiteBirds (Aves) Are A Group Of: WingsGabriel Angelo AbrauNoch keine Bewertungen
- Rosenberg Et Al - Through Interpreters' Eyes, Comparing Roles of Professional and Family InterpretersDokument7 SeitenRosenberg Et Al - Through Interpreters' Eyes, Comparing Roles of Professional and Family InterpretersMaria AguilarNoch keine Bewertungen
- Grade 7 1ST Quarter ExamDokument3 SeitenGrade 7 1ST Quarter ExamJay Haryl PesalbonNoch keine Bewertungen
- CSEC Eng A Summary ExerciseDokument1 SeiteCSEC Eng A Summary ExerciseArisha NicholsNoch keine Bewertungen
- Chapter 8 - FluidDokument26 SeitenChapter 8 - FluidMuhammad Aminnur Hasmin B. HasminNoch keine Bewertungen
- BHP Billiton Foundations For Graduates Program Brochure 2012Dokument4 SeitenBHP Billiton Foundations For Graduates Program Brochure 2012JulchairulNoch keine Bewertungen
- Seismic Response of Elevated Liquid Storage Steel Tanks Isolated by VCFPS at Top of Tower Under Near-Fault Ground MotionsDokument6 SeitenSeismic Response of Elevated Liquid Storage Steel Tanks Isolated by VCFPS at Top of Tower Under Near-Fault Ground MotionsciscoNoch keine Bewertungen
- English Lesson Plan 6 AugustDokument10 SeitenEnglish Lesson Plan 6 AugustKhairunnisa FazilNoch keine Bewertungen
- Administrator's Guide: SeriesDokument64 SeitenAdministrator's Guide: SeriesSunny SaahilNoch keine Bewertungen
- Gits Systems Anaphy DisordersDokument23 SeitenGits Systems Anaphy DisordersIlawNoch keine Bewertungen
- (Abhijit Champanerkar, Oliver Dasbach, Efstratia K (B-Ok - Xyz)Dokument273 Seiten(Abhijit Champanerkar, Oliver Dasbach, Efstratia K (B-Ok - Xyz)gogNoch keine Bewertungen