Das könnte Ihnen auch gefallen
- Nomenclature and Classification of Lumbar Disk PathologyDokument21 SeitenNomenclature and Classification of Lumbar Disk PathologyYasemen KNoch keine Bewertungen
- JNC 8 Guideline Algorithm for Treating HypertensionDokument2 SeitenJNC 8 Guideline Algorithm for Treating HypertensionTaradifaNurInsi0% (1)
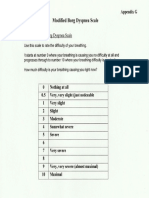
- Borg Scale PDFDokument1 SeiteBorg Scale PDFNoor FadhilaNoch keine Bewertungen
- Dietary Supplements and Functional Foods 2 Sides of A Coin PDFDokument7 SeitenDietary Supplements and Functional Foods 2 Sides of A Coin PDFNoor FadhilaNoch keine Bewertungen
- Garlic Increases Antioxidant Levels in Diabetic and HypertenDokument7 SeitenGarlic Increases Antioxidant Levels in Diabetic and HypertenAndrew NugrohoNoch keine Bewertungen
- STR 0000000000000069 FullDokument34 SeitenSTR 0000000000000069 FullcignalNoch keine Bewertungen
- Appendix 1 Quick Guide To Herb-Drug InteractionsDokument11 SeitenAppendix 1 Quick Guide To Herb-Drug InteractionsNoor FadhilaNoch keine Bewertungen
- Benefits, Adverse Effects and Drug Interactions of Herbal TH PDFDokument15 SeitenBenefits, Adverse Effects and Drug Interactions of Herbal TH PDFNoor FadhilaNoch keine Bewertungen
- 1 - Modified Ashworth Scale PDFDokument1 Seite1 - Modified Ashworth Scale PDFNoor FadhilaNoch keine Bewertungen
- Cell Membrane Damage and Protein Interaction Induced by CopperDokument11 SeitenCell Membrane Damage and Protein Interaction Induced by CopperNoor FadhilaNoch keine Bewertungen
- In Vitro Interactions of Water-Soluble Garlic Components Wit PDFDokument4 SeitenIn Vitro Interactions of Water-Soluble Garlic Components Wit PDFNoor FadhilaNoch keine Bewertungen
- Borg Scale PDFDokument1 SeiteBorg Scale PDFNoor FadhilaNoch keine Bewertungen
- Sensitivitas AntibiotikDokument4 SeitenSensitivitas AntibiotikNoor FadhilaNoch keine Bewertungen
- Eng PDFDokument34 SeitenEng PDFAkbar RihansyahNoch keine Bewertungen
- Fenton2013growthchartcolor Boys PDFDokument1 SeiteFenton2013growthchartcolor Boys PDFNoor FadhilaNoch keine Bewertungen
- Inhibition Properties of Propolis Extracts To Some Clinically Important EnzymesDokument5 SeitenInhibition Properties of Propolis Extracts To Some Clinically Important EnzymesNoor FadhilaNoch keine Bewertungen
- Tetralogy of FallotDokument5 SeitenTetralogy of FallotNoor FadhilaNoch keine Bewertungen
- 1 - Modified Ashworth Scale PDFDokument1 Seite1 - Modified Ashworth Scale PDFNoor FadhilaNoch keine Bewertungen
- Lirik Lagu Adele - Someone Like You LyricsDokument3 SeitenLirik Lagu Adele - Someone Like You LyricsNoor FadhilaNoch keine Bewertungen
- Borg ScaleDokument1 SeiteBorg ScaleNoor FadhilaNoch keine Bewertungen
- Pulpitis: A ReviewDokument6 SeitenPulpitis: A ReviewIOSRjournalNoch keine Bewertungen
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (890)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (399)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (344)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (587)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (73)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (265)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2219)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (119)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- Lightspeed VCT XT: Ge HealthcareDokument4 SeitenLightspeed VCT XT: Ge HealthcareВалерий КоваленкоNoch keine Bewertungen
- DSE4610 DSE4620 Operators Manual PDFDokument86 SeitenDSE4610 DSE4620 Operators Manual PDFChristopher100% (3)
- Blunt Chest TraumaDokument7 SeitenBlunt Chest TraumaCatherine MorrisNoch keine Bewertungen
- Comparison Between Traditional 2-Dimensional Cephalometry and A 3-Dimensional Approach On Human Dry SkullsDokument13 SeitenComparison Between Traditional 2-Dimensional Cephalometry and A 3-Dimensional Approach On Human Dry SkullsMarllury PabonNoch keine Bewertungen
- Managing Adnexal Masses in PregnancyDokument6 SeitenManaging Adnexal Masses in PregnancyRosália Coutada100% (1)
- Aruba TrialDokument8 SeitenAruba TrialPatty RiveraNoch keine Bewertungen
- BSC - RADIOLOGY Syllabus-7 ModulesDokument35 SeitenBSC - RADIOLOGY Syllabus-7 Modulesagoyal5145Noch keine Bewertungen
- MaxMed 2023 SILVER GROUP TOB Category CDokument14 SeitenMaxMed 2023 SILVER GROUP TOB Category Cbaashii4Noch keine Bewertungen
- Assessing HepatomegalyDokument11 SeitenAssessing HepatomegalyIndi AndiniNoch keine Bewertungen
- ARTIS Zee Brochure 10 2019Dokument40 SeitenARTIS Zee Brochure 10 2019Naoufel AbbesNoch keine Bewertungen
- Nuctech WooKong HDokument2 SeitenNuctech WooKong HJonathan ChikNoch keine Bewertungen
- Contribution of Muscle MRI For Diagnosis of MyopathyDokument20 SeitenContribution of Muscle MRI For Diagnosis of MyopathyJose EdgarNoch keine Bewertungen
- Medical TerminologyDokument107 SeitenMedical TerminologyonmcvNoch keine Bewertungen
- Brain Haemorrhage Segmentation Using Discrete Wavelet TransformDokument5 SeitenBrain Haemorrhage Segmentation Using Discrete Wavelet TransformIJIRAE- International Journal of Innovative Research in Advanced EngineeringNoch keine Bewertungen
- RT05 - EBT1 - Sources - Techniques WEBDokument89 SeitenRT05 - EBT1 - Sources - Techniques WEBMahendra KusumaNoch keine Bewertungen
- Pencitraan KepalaDokument38 SeitenPencitraan KepalajunsukyokoNoch keine Bewertungen
- Cone Beam PAI Estrela Et Al 2008Dokument7 SeitenCone Beam PAI Estrela Et Al 2008Surya WijayaNoch keine Bewertungen
- Aviation Security AbbreviationsDokument13 SeitenAviation Security Abbreviationssurajit karmakar100% (1)
- Radiography HandbookDokument51 SeitenRadiography Handbookjoan carlos casadoNoch keine Bewertungen
- Pet MriDokument165 SeitenPet MriAzmal Kabir SarkerNoch keine Bewertungen
- Dynamic Testing of Generator Protection Using Model PlatformDokument20 SeitenDynamic Testing of Generator Protection Using Model PlatformVignesh RajendranNoch keine Bewertungen
- TestBlock - ETB-14Dokument8 SeitenTestBlock - ETB-14rudyplNoch keine Bewertungen
- Pemeriksaan Radiologi Trauma ThoraxDokument6 SeitenPemeriksaan Radiologi Trauma ThoraxshabrinaNoch keine Bewertungen
- CT ScanDokument37 SeitenCT ScanBayu Ihkshan Yamada TriatmojoNoch keine Bewertungen
- Toshiba Aquilion 16CT ScannerDokument5 SeitenToshiba Aquilion 16CT ScannerDavid PuyóNoch keine Bewertungen
- Atlas of Normal Radiographic Anatomy and Anatomic Variants in The Dog and CatDokument311 SeitenAtlas of Normal Radiographic Anatomy and Anatomic Variants in The Dog and CatBinkyMiau100% (1)
- Academy of Life Underwriting - ALU 101 - Basic Life Insurance Underwriting - Textbook For 2022 Exam Cycle (2021)Dokument359 SeitenAcademy of Life Underwriting - ALU 101 - Basic Life Insurance Underwriting - Textbook For 2022 Exam Cycle (2021)KALPESH SHAHNoch keine Bewertungen
- Retro-Orbital Injections in MiceDokument6 SeitenRetro-Orbital Injections in MiceFrancisco Ibañez IrribarraNoch keine Bewertungen
- 5 Radiology CT Scan and MRIDokument9 Seiten5 Radiology CT Scan and MRIAbegail IbañezNoch keine Bewertungen
- Trigonometric Functions Relate To MedicineDokument10 SeitenTrigonometric Functions Relate To MedicineJanlie GautaneNoch keine Bewertungen