Das könnte Ihnen auch gefallen
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (894)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (587)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (344)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (119)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (399)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2219)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (265)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (73)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- MCU 2015 ERS Practical Handbook of Noninvasive VentilationDokument320 SeitenMCU 2015 ERS Practical Handbook of Noninvasive VentilationAlina CiubotariuNoch keine Bewertungen
- Essential steps and complications of endotracheal intubationDokument25 SeitenEssential steps and complications of endotracheal intubationAdeel Rana100% (1)
- (RS) Pneumonia With Severe HypoxiaDokument4 Seiten(RS) Pneumonia With Severe Hypoxiaapi-3769252100% (2)
- The New Blast Results Page: ScopeDokument4 SeitenThe New Blast Results Page: ScopePattyNoch keine Bewertungen
- Intramembranous and endochondral ossification processesDokument8 SeitenIntramembranous and endochondral ossification processesMuhammad SaifullohNoch keine Bewertungen
- The New Blast Results Page: ScopeDokument4 SeitenThe New Blast Results Page: ScopePattyNoch keine Bewertungen
- Intramembranous and endochondral ossification processesDokument8 SeitenIntramembranous and endochondral ossification processesMuhammad SaifullohNoch keine Bewertungen
- The New Blast Results Page: ScopeDokument4 SeitenThe New Blast Results Page: ScopePattyNoch keine Bewertungen
- Notes 191123 121756 607 PDFDokument3 SeitenNotes 191123 121756 607 PDFMuhammad SaifullohNoch keine Bewertungen
- Skipping Breakfast and 5-Year Changes in Body Mass Index and Waist Circumference in Japanese Men and Women PDFDokument18 SeitenSkipping Breakfast and 5-Year Changes in Body Mass Index and Waist Circumference in Japanese Men and Women PDFMuhammad SaifullohNoch keine Bewertungen
- Skipping Breakfast and 5-Year Changes in Body Mass Index and Waist Circumference in Japanese Men and Women PDFDokument18 SeitenSkipping Breakfast and 5-Year Changes in Body Mass Index and Waist Circumference in Japanese Men and Women PDFMuhammad SaifullohNoch keine Bewertungen
- Stem Cell (3), BB-Ida PDFDokument50 SeitenStem Cell (3), BB-Ida PDFMuhammad SaifullohNoch keine Bewertungen
- 2Dokument14 Seiten2Muhammad SaifullohNoch keine Bewertungen
- Introduction For Medical Doctor: (Soon To Be)Dokument87 SeitenIntroduction For Medical Doctor: (Soon To Be)Muhammad SaifullohNoch keine Bewertungen
- LulDokument5 SeitenLulMuhammad SaifullohNoch keine Bewertungen
- 3Dokument9 Seiten3Muhammad SaifullohNoch keine Bewertungen
- 5Dokument3 Seiten5Muhammad SaifullohNoch keine Bewertungen
- 1Dokument11 Seiten1Muhammad SaifullohNoch keine Bewertungen
- 5Dokument3 Seiten5Muhammad SaifullohNoch keine Bewertungen
- Alpha-1-Antitrypsin DeficiencyDokument13 SeitenAlpha-1-Antitrypsin DeficiencyMuhammad SaifullohNoch keine Bewertungen
- Playing Video Games Linked To AsthmaDokument3 SeitenPlaying Video Games Linked To AsthmaMuhammad SaifullohNoch keine Bewertungen
- Booklet Atc Pps PDFDokument37 SeitenBooklet Atc Pps PDFGrudi JordanovNoch keine Bewertungen
- Hbsc3203 Chemistry II Full Version Reading BrickDokument324 SeitenHbsc3203 Chemistry II Full Version Reading BrickAisyah NazifahNoch keine Bewertungen
- 10 Imp English Grammer Value Based Type 9Dokument7 Seiten10 Imp English Grammer Value Based Type 9Aaradhy TiwariNoch keine Bewertungen
- Respiratory System: Gas ExchangeDokument28 SeitenRespiratory System: Gas ExchangePinaka ShungaNoch keine Bewertungen
- Activity Worksheet.9 ScienceDokument5 SeitenActivity Worksheet.9 Sciencelavenia acdalNoch keine Bewertungen
- PneumoniaDokument41 SeitenPneumoniapaanar100% (2)
- Question Bank For Telangana State Board BiologyDokument105 SeitenQuestion Bank For Telangana State Board BiologyChetan JainNoch keine Bewertungen
- Case Study of PneumoniaDokument8 SeitenCase Study of PneumoniaAnne SedanzaNoch keine Bewertungen
- NCP Impaired Gas ExchangeDokument2 SeitenNCP Impaired Gas ExchangeCharissa Magistrado De LeonNoch keine Bewertungen
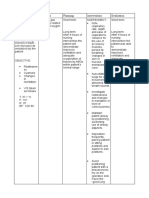
- Epiglottitis: Assessment Nursing Diagnosis Scientific Explanatio N Planning Nursing Intervention Rationale EvaluationDokument3 SeitenEpiglottitis: Assessment Nursing Diagnosis Scientific Explanatio N Planning Nursing Intervention Rationale EvaluationfifiNoch keine Bewertungen
- Indication For IntubationDokument4 SeitenIndication For IntubationwisanggeniNoch keine Bewertungen
- Unit V Pulmonary NursingDokument22 SeitenUnit V Pulmonary Nursingtamtamtamtama0Noch keine Bewertungen
- 1-Mechanism and Regulation of Respiration ModifiedDokument10 Seiten1-Mechanism and Regulation of Respiration Modifiedخالد القرشيNoch keine Bewertungen
- 5.1 OB-Pulmonary Disorders in Pregnancy (Dr. Bautista)Dokument10 Seiten5.1 OB-Pulmonary Disorders in Pregnancy (Dr. Bautista)Monique BorresNoch keine Bewertungen
- Noninvasive Ventilator Devices and ModesDokument11 SeitenNoninvasive Ventilator Devices and ModesISABEL SOFIA CABARCAS COGOLLONoch keine Bewertungen
- Material Safety Data Sheet MSDS NR:: Calcium Oxide CO001Dokument5 SeitenMaterial Safety Data Sheet MSDS NR:: Calcium Oxide CO001mohdsuhail2k3055Noch keine Bewertungen
- Respiratory Distress SyndromeDokument30 SeitenRespiratory Distress SyndromeDennis MiritiNoch keine Bewertungen
- Campbell 796Dokument2 SeitenCampbell 796ANG BENG KANG MoeNoch keine Bewertungen
- Post-natal Care After Elective LSCSDokument44 SeitenPost-natal Care After Elective LSCSpriyanka100% (2)
- Asthma Bio142 LTADokument2 SeitenAsthma Bio142 LTAKate MckinneyNoch keine Bewertungen
- Nurse sees post-op appendectomy client first after endorsementDokument9 SeitenNurse sees post-op appendectomy client first after endorsementMishia Renee EchonNoch keine Bewertungen
- Mechanical Ventilation:: 2. Positive Pressure VentilatorDokument3 SeitenMechanical Ventilation:: 2. Positive Pressure VentilatorMurad KhairoNoch keine Bewertungen
- Disease ProjectDokument18 SeitenDisease Projectapi-293515530Noch keine Bewertungen
- ACFrOgDACnKE0rUjf42HXaSb36Wbju Urd7BPPqmTBRXMMFtZ91-fOr1fErSfh6BzXghJFKNYiKG5H-y3ET76l8IkKipRRxFa4B6gSp0OP6njH7C 5ulv8f C1cL DaDokument209 SeitenACFrOgDACnKE0rUjf42HXaSb36Wbju Urd7BPPqmTBRXMMFtZ91-fOr1fErSfh6BzXghJFKNYiKG5H-y3ET76l8IkKipRRxFa4B6gSp0OP6njH7C 5ulv8f C1cL Dajelena_stankovic_34Noch keine Bewertungen
- Ib Bio Previous IB Exam Essay QuestionsDokument34 SeitenIb Bio Previous IB Exam Essay Questionssrahimi@verizon.net100% (2)
- 1 Label The Diagram Below.: Chapter 1: RespirationDokument10 Seiten1 Label The Diagram Below.: Chapter 1: RespirationNuzul HaikalNoch keine Bewertungen
- 05.12 Anatomy of The Larynx & Physiology of PhonationDokument30 Seiten05.12 Anatomy of The Larynx & Physiology of PhonationReg LagartejaNoch keine Bewertungen