Das könnte Ihnen auch gefallen
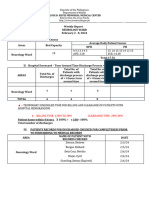
- Weekly Report Feb. 2-8, 2024Dokument8 SeitenWeekly Report Feb. 2-8, 2024vandiemagallanesNoch keine Bewertungen
- Cioms FormDokument2 SeitenCioms Formnaura_farrelNoch keine Bewertungen
- Case Study FormatDokument4 SeitenCase Study FormatLuiezt BernardoNoch keine Bewertungen
- Case Study Format 1Dokument4 SeitenCase Study Format 1Michelle Rose RodaviaNoch keine Bewertungen
- Brief Description of The Disease/statistical IncidenceDokument2 SeitenBrief Description of The Disease/statistical IncidenceLeanne Princess Gamboa100% (1)
- Health Emergency Preparedness Response and Recovery PlanDokument11 SeitenHealth Emergency Preparedness Response and Recovery PlanReslyn YanocNoch keine Bewertungen
- Pedia Case Study FormatDokument4 SeitenPedia Case Study FormatJohn Carlo B. Dungca100% (1)
- CBAHI and JCI Common Asked Questions. 2023Dokument5 SeitenCBAHI and JCI Common Asked Questions. 2023Rini NoviantiNoch keine Bewertungen
- Head Nursing: University of Cebu - BaniladDokument30 SeitenHead Nursing: University of Cebu - BaniladVjay DingNoch keine Bewertungen
- Lic 602 ADokument6 SeitenLic 602 ALm RappeportNoch keine Bewertungen
- Check List For SNCUDokument5 SeitenCheck List For SNCUpriyahospitalNoch keine Bewertungen
- GNO Medication ReviewDokument18 SeitenGNO Medication ReviewCHARLENE MAY PANDINONoch keine Bewertungen
- Case Study FormatDokument4 SeitenCase Study FormatKOBE TOMAGANNoch keine Bewertungen
- Medical Plan ICS 206Dokument3 SeitenMedical Plan ICS 206RexNoch keine Bewertungen
- Medical Record Dept.Dokument32 SeitenMedical Record Dept.Kool KingNoch keine Bewertungen
- VBA-21-0960G-4-ARE Intestinal Surgery PDFDokument3 SeitenVBA-21-0960G-4-ARE Intestinal Surgery PDFCombat CraigNoch keine Bewertungen
- Perioperative Pre-Class Mini-Lecture - CH 17-19Dokument22 SeitenPerioperative Pre-Class Mini-Lecture - CH 17-19Marcel YoungNoch keine Bewertungen
- Duty NotesDokument4 SeitenDuty NotesjustinjareddNoch keine Bewertungen
- 9 Caf001diDokument1 Seite9 Caf001diwhite304Noch keine Bewertungen
- Clinical Case Study Format General Ward 1Dokument3 SeitenClinical Case Study Format General Ward 1Fita ClanNoch keine Bewertungen
- DJPRH Processes and ProceduresDokument289 SeitenDJPRH Processes and ProceduresjeffaguilarNoch keine Bewertungen
- Medical Plan ICS 206Dokument3 SeitenMedical Plan ICS 206Leo ConstantinoNoch keine Bewertungen
- Signed DOH-DBM Joint Circular On One COVID-19 Allowance (OCA) OCA Information System (OCAIS)Dokument35 SeitenSigned DOH-DBM Joint Circular On One COVID-19 Allowance (OCA) OCA Information System (OCAIS)genNoch keine Bewertungen
- Project Proposal: Code of 1991 Mandates The Local Government Units To Provide Basic FacilitiesDokument4 SeitenProject Proposal: Code of 1991 Mandates The Local Government Units To Provide Basic Facilitiescasagantm-1Noch keine Bewertungen
- VA Housebound Form VBA-21-2680Dokument2 SeitenVA Housebound Form VBA-21-2680tom2susanNoch keine Bewertungen
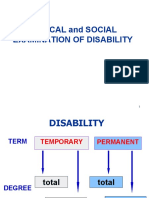
- Medical and Social Examination of DisabilityDokument20 SeitenMedical and Social Examination of DisabilityashighaNoch keine Bewertungen
- Health Record GuidelinesDokument18 SeitenHealth Record GuidelinesragNoch keine Bewertungen
- Source NP%Dokument10 SeitenSource NP%Ima Leigh RubioNoch keine Bewertungen
- Dictation Discharge Summary TemplateDokument19 SeitenDictation Discharge Summary TemplateBobby ReddyNoch keine Bewertungen
- Grand Case Presentation FormatDokument7 SeitenGrand Case Presentation FormatRENEROSE TORRESNoch keine Bewertungen
- Quiz Hospital DocumentationDokument5 SeitenQuiz Hospital DocumentationJessica EdiosNoch keine Bewertungen
- Customer Satisfction - Quarter ReportDokument3 SeitenCustomer Satisfction - Quarter Reportjimelyquinones78Noch keine Bewertungen
- Surgical Case Presentation SchemeDokument4 SeitenSurgical Case Presentation SchemeVasilescu LauraNoch keine Bewertungen
- New Assessment Tool For Hospitals (Repaired)Dokument60 SeitenNew Assessment Tool For Hospitals (Repaired)Ana dominique Hernandez100% (1)
- 2021 AMR - CoacoDokument11 Seiten2021 AMR - CoacoAngelo MojicaNoch keine Bewertungen
- Far Eastern University Institute of Nursing: Individual/ Group Nursing Process FormatDokument8 SeitenFar Eastern University Institute of Nursing: Individual/ Group Nursing Process FormatAbie Jewel Joy RoqueNoch keine Bewertungen
- Medical-Surgical Nursing Knowledge & Skills ChecklistDokument3 SeitenMedical-Surgical Nursing Knowledge & Skills Checklistnorthweststaffing100% (1)
- Digital Learner'S Worksheet: Student Nameraphael Chino Aragon Date: InstitutionDokument67 SeitenDigital Learner'S Worksheet: Student Nameraphael Chino Aragon Date: InstitutionRAPHAEL CHINO ARAGONNoch keine Bewertungen
- Nurse Np1 Board CramsheetDokument8 SeitenNurse Np1 Board CramsheetZero TwoNoch keine Bewertungen
- Activity On Hospital Documentation - HospPharmLab Act 1Dokument4 SeitenActivity On Hospital Documentation - HospPharmLab Act 1Jan Aerielle AzulNoch keine Bewertungen
- 5 6212887793887085843 PDFDokument11 Seiten5 6212887793887085843 PDFeruditeNoch keine Bewertungen
- Missionary Recommendation Physician Dental FormDokument5 SeitenMissionary Recommendation Physician Dental FormdozieojiakuNoch keine Bewertungen
- VBA-21-0960J-3-ARE Prostate Cancer PDFDokument3 SeitenVBA-21-0960J-3-ARE Prostate Cancer PDFCombat CraigNoch keine Bewertungen
- Case Study FormatDokument2 SeitenCase Study Formatgrandpa12Noch keine Bewertungen
- West Visayas State University Medical Center E. Lopez St. Jaro Iloilo CityDokument7 SeitenWest Visayas State University Medical Center E. Lopez St. Jaro Iloilo CityRegine Marie EspañaNoch keine Bewertungen
- Safe HospitalDokument36 SeitenSafe HospitalSagrina BangunNoch keine Bewertungen
- Nursing Recruitment Skills Checklist: Guidance or DirectionDokument4 SeitenNursing Recruitment Skills Checklist: Guidance or DirectionKRIZZEL CATAMINNoch keine Bewertungen
- ALJ Decision Holy Cross 05-CA-182154 - 07212017Dokument30 SeitenALJ Decision Holy Cross 05-CA-182154 - 07212017David LublinNoch keine Bewertungen
- Hiv and Aids OrientationDokument56 SeitenHiv and Aids OrientationRufo JawaNoch keine Bewertungen
- ESR Follow-Up FormDokument2 SeitenESR Follow-Up FormAflkjael JamaelNoch keine Bewertungen
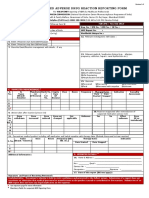
- ADRnewReporting Form 1.4Dokument2 SeitenADRnewReporting Form 1.4Sourabh kundara0% (1)
- Severe Acute Malnutrition Guidelines - PPD - CPDDokument7 SeitenSevere Acute Malnutrition Guidelines - PPD - CPDTamal Deb BarmaNoch keine Bewertungen
- Esr Summary 2023Dokument2 SeitenEsr Summary 2023Mohamed KamalNoch keine Bewertungen
- Health Facilities and Services Regulatory Bureau: Republic of The Philippines Department of HealthDokument60 SeitenHealth Facilities and Services Regulatory Bureau: Republic of The Philippines Department of HealthMichael Capuyan JrNoch keine Bewertungen
- NDRRMC - 206Dokument3 SeitenNDRRMC - 206Dexter Martije DescotidoNoch keine Bewertungen
- Nursing Health History FormatDokument7 SeitenNursing Health History FormatJasmine PonceNoch keine Bewertungen
- Nursing Health History FormatDokument7 SeitenNursing Health History Formatgeraldine suarezNoch keine Bewertungen
- Syllab Ccincommhealthcare-20042021Dokument23 SeitenSyllab Ccincommhealthcare-20042021Suresh JNoch keine Bewertungen
- Good Health in the Tropics: Advice to Travellers and SettlersVon EverandGood Health in the Tropics: Advice to Travellers and SettlersNoch keine Bewertungen
- Plant Disease: An Advanced Treatise: How Plants Suffer from DiseaseVon EverandPlant Disease: An Advanced Treatise: How Plants Suffer from DiseaseJames G. HorsfallNoch keine Bewertungen
- HL 2022 Sample PagesDokument14 SeitenHL 2022 Sample PagesJános JuhászNoch keine Bewertungen
- Mindmanager Enterprise: Promotes Collaborative Working Practices at ManeDokument2 SeitenMindmanager Enterprise: Promotes Collaborative Working Practices at ManeJose M. GuerreroNoch keine Bewertungen
- Lions Mane Ultimate Guide 00Dokument1 SeiteLions Mane Ultimate Guide 00János JuhászNoch keine Bewertungen
- Ps 2Dokument6 SeitenPs 2János JuhászNoch keine Bewertungen
- Fen-11 User ManualDokument40 SeitenFen-11 User ManualJuan Jiménez GamezNoch keine Bewertungen
- Manual Nintendo64 SinAndPunishment ENDokument11 SeitenManual Nintendo64 SinAndPunishment ENJános JuhászNoch keine Bewertungen
- En FEN 01 Um CDokument32 SeitenEn FEN 01 Um CJános JuhászNoch keine Bewertungen
- SYLLABUS For JEE (Main) - 2021 Syllabus For Paper-1Dokument19 SeitenSYLLABUS For JEE (Main) - 2021 Syllabus For Paper-1HrishiNoch keine Bewertungen
- Pri PDFDokument5 SeitenPri PDFAnonymous dyqQV3Noch keine Bewertungen
- D2.2a Poor FenDokument9 SeitenD2.2a Poor FenJános JuhászNoch keine Bewertungen
- Human MAIT Cells Are Devoid of Alloreactive Potential: Prompting Their Use As Universal Cells For Adoptive Immune TherapyDokument34 SeitenHuman MAIT Cells Are Devoid of Alloreactive Potential: Prompting Their Use As Universal Cells For Adoptive Immune TherapyJános JuhászNoch keine Bewertungen
- Check MAIT: References Cites 53 ArticlesDokument7 SeitenCheck MAIT: References Cites 53 ArticlesJános JuhászNoch keine Bewertungen
- Ids High-Leit Flyer enDokument8 SeitenIds High-Leit Flyer enJános JuhászNoch keine Bewertungen
- Ding Dong Merrily On HighDokument1 SeiteDing Dong Merrily On Highpfr31430Noch keine Bewertungen
- Cancers: MAIT Cells: Partners or Enemies in Cancer Immunotherapy?Dokument23 SeitenCancers: MAIT Cells: Partners or Enemies in Cancer Immunotherapy?János JuhászNoch keine Bewertungen
- BasicRiderCourse HandbookDokument84 SeitenBasicRiderCourse HandbookKonstantinos AirmanNoch keine Bewertungen
- The RISC Algorithm Language (RISCAL)Dokument155 SeitenThe RISC Algorithm Language (RISCAL)János JuhászNoch keine Bewertungen
- Giuseppe Verdi - Aida MARCIA TRIONFALEDokument38 SeitenGiuseppe Verdi - Aida MARCIA TRIONFALEJános JuhászNoch keine Bewertungen
- Prupersonal Accident EBrochure EnglishDokument6 SeitenPrupersonal Accident EBrochure EnglishJános JuhászNoch keine Bewertungen
- PRI FrenchEnergyTransitionLawDokument16 SeitenPRI FrenchEnergyTransitionLawJános JuhászNoch keine Bewertungen
- SAMv 1Dokument21 SeitenSAMv 1János JuhászNoch keine Bewertungen
- PumpingStationOne20140628 Real TimeProgrammingWithBeagleBonePRUsDokument37 SeitenPumpingStationOne20140628 Real TimeProgrammingWithBeagleBonePRUsJános JuhászNoch keine Bewertungen
- INVM11630Dokument36 SeitenINVM11630János JuhászNoch keine Bewertungen
- A Step-By-Step Guide To The Prufund Smoothing ProcessDokument6 SeitenA Step-By-Step Guide To The Prufund Smoothing ProcessJános JuhászNoch keine Bewertungen
- Pru Ar2016 FullDokument412 SeitenPru Ar2016 FullEsplanadeNoch keine Bewertungen
- PRU Assembly Instruction User GuideDokument50 SeitenPRU Assembly Instruction User GuideJános JuhászNoch keine Bewertungen
- The Prufund Range of Funds: An Introduction ToDokument24 SeitenThe Prufund Range of Funds: An Introduction ToJános JuhászNoch keine Bewertungen
- INVB6572Dokument24 SeitenINVB6572János JuhászNoch keine Bewertungen
- CV 2017 VirginiaDokument4 SeitenCV 2017 Virginiaapi-353693776Noch keine Bewertungen
- Porcelain Veneer Preparations PDFDokument3 SeitenPorcelain Veneer Preparations PDFSamah FadelNoch keine Bewertungen
- Diagnosis and Management of Meniscal Injury: PresentationDokument4 SeitenDiagnosis and Management of Meniscal Injury: PresentationemilyNoch keine Bewertungen
- Echo Facts IndexDokument3 SeitenEcho Facts Indexs336336anl100% (1)
- NCP Acute PainDokument2 SeitenNCP Acute PainNecheal BaayNoch keine Bewertungen
- Valleylab ForceTriad - User Manual PDFDokument100 SeitenValleylab ForceTriad - User Manual PDFPaulina LekszyckaNoch keine Bewertungen
- InjectionsDokument26 SeitenInjectionsNotInterested100% (3)
- Psych Units 11-13 Cheat SheetDokument1 SeitePsych Units 11-13 Cheat SheetTalia ShumanNoch keine Bewertungen
- Failure Mode and Effect Analysis (FMEA) Sanglah General Hospital 2012Dokument28 SeitenFailure Mode and Effect Analysis (FMEA) Sanglah General Hospital 2012ferekonstantinusNoch keine Bewertungen
- Pe StressDokument50 SeitenPe StressAngelica OrbizoNoch keine Bewertungen
- Tourette Syndrome Script FinalDokument5 SeitenTourette Syndrome Script Finalapi-439171422Noch keine Bewertungen
- 02 Full Crown PreparationDokument35 Seiten02 Full Crown PreparationSurgaBetariJelita100% (1)
- Drug Interactions Results - MICROMEDEX®Dokument3 SeitenDrug Interactions Results - MICROMEDEX®Kike MenesesNoch keine Bewertungen
- Emergency Protocol ProcedureDokument14 SeitenEmergency Protocol Procedurejmmos207064Noch keine Bewertungen
- Hystori of EndoskopikDokument3 SeitenHystori of Endoskopiksmansa123Noch keine Bewertungen
- Skin Care PowerpointDokument52 SeitenSkin Care Powerpointisapatrick812667% (3)
- Smaple Case Study - Virginia's Henderson Need Theory PDFDokument8 SeitenSmaple Case Study - Virginia's Henderson Need Theory PDFEduardo AnerdezNoch keine Bewertungen
- Nursing Care Plan Breast-CancerDokument2 SeitenNursing Care Plan Breast-CancerGreg Llandelar100% (2)
- Trauma Wajah Tutorial - PPTX RevDokument49 SeitenTrauma Wajah Tutorial - PPTX RevShinta Andi SarasatiNoch keine Bewertungen
- Adl IadlDokument20 SeitenAdl IadlKrisna Eka Yudha100% (1)
- Pharyngeal ReflexDokument3 SeitenPharyngeal ReflexAyra Nakrish AlvarezNoch keine Bewertungen
- Kyp Ho Scoliosis 1Dokument70 SeitenKyp Ho Scoliosis 1Tias DiahNoch keine Bewertungen
- Chronic Kidney Disease in Children Clinical PresentationDokument4 SeitenChronic Kidney Disease in Children Clinical PresentationJendriella LaaeeNoch keine Bewertungen
- Insulin Adjustment Workbook CompleteDokument53 SeitenInsulin Adjustment Workbook CompleteDiabestes-stuff100% (1)
- Suggamadex Remifentanyl PalonosetronDokument28 SeitenSuggamadex Remifentanyl PalonosetronSai TejeswiNoch keine Bewertungen
- RETDEM TEMPLATE AutoRecoveredDokument5 SeitenRETDEM TEMPLATE AutoRecoveredAlexa Gwen Agnila BihagNoch keine Bewertungen
- How To Perform A Head To Toe AssessmentDokument2 SeitenHow To Perform A Head To Toe AssessmentLalaine RomeroNoch keine Bewertungen
- NaloxoneDokument3 SeitenNaloxoneTracyNoch keine Bewertungen
- Fibrous Dysplasia of BoneDokument31 SeitenFibrous Dysplasia of Bonet.babyNoch keine Bewertungen
- Understanding Neurology - A Problem-Orientated Approach PDFDokument241 SeitenUnderstanding Neurology - A Problem-Orientated Approach PDFAshabul AnharNoch keine Bewertungen