Das könnte Ihnen auch gefallen
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (399)
- NumberDokument1 SeiteNumberMeutia SavitriNoch keine Bewertungen
- Neutrofils in Post Myocardial Infarction InflammationDokument9 SeitenNeutrofils in Post Myocardial Infarction InflammationMeutia SavitriNoch keine Bewertungen
- ReflexesDokument37 SeitenReflexesMeutia SavitriNoch keine Bewertungen
- Arthritis SepsisDokument6 SeitenArthritis SepsisMeutia SavitriNoch keine Bewertungen
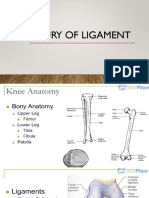
- Injury of LigamentDokument17 SeitenInjury of LigamentMeutia SavitriNoch keine Bewertungen
- Ewing's SarcomaDokument8 SeitenEwing's SarcomaMeutia SavitriNoch keine Bewertungen
- Plenary Discussion Week 3: Group of 15-CDokument143 SeitenPlenary Discussion Week 3: Group of 15-CMeutia SavitriNoch keine Bewertungen
- LCPD Bahasa InggrisDokument10 SeitenLCPD Bahasa InggrisMeutia SavitriNoch keine Bewertungen
- LCPD Bahasa InggrisDokument10 SeitenLCPD Bahasa InggrisMeutia SavitriNoch keine Bewertungen
- Tumor PenisDokument9 SeitenTumor PenisMeutia Savitri100% (1)
- Stimulation of Children DevelopmentDokument12 SeitenStimulation of Children DevelopmentMeutia SavitriNoch keine Bewertungen
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (894)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (587)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (265)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (73)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (119)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- Immunology & Serology: Preliminaries: Romie Solacito, MLS3CDokument12 SeitenImmunology & Serology: Preliminaries: Romie Solacito, MLS3CRomie Solacito100% (2)
- S1 Spike Protein Causes PASC, Cytokine Storm, & Long COVIDDokument115 SeitenS1 Spike Protein Causes PASC, Cytokine Storm, & Long COVIDAnthony DocKek PenaNoch keine Bewertungen
- The Biology of Scar FormationDokument11 SeitenThe Biology of Scar FormationOscar Barrios BravoNoch keine Bewertungen
- Dr. Dwi Ngestiningsih - Penurunan Imunitas Lansia+LOGO BARUDokument27 SeitenDr. Dwi Ngestiningsih - Penurunan Imunitas Lansia+LOGO BARUMuhammad Zul Fahmi AkbarNoch keine Bewertungen
- Pre-Medical Division: Immunity and DiseaseDokument55 SeitenPre-Medical Division: Immunity and DiseaseAravind RaoNoch keine Bewertungen
- 1.inflammation & Repair: Cardinal Signs of InflammationDokument47 Seiten1.inflammation & Repair: Cardinal Signs of Inflammationsharu4291Noch keine Bewertungen
- Textbook of Diagnostic Microbiology 4th Edition Mahon Test BankDokument13 SeitenTextbook of Diagnostic Microbiology 4th Edition Mahon Test Banklaylafarleyh3i8j9100% (25)
- Lesson Plan Immunity and DiseasesDokument11 SeitenLesson Plan Immunity and DiseasesAnalyn ValentinNoch keine Bewertungen
- Tuberculosis - StatPearls - NCBI BookshelfDokument10 SeitenTuberculosis - StatPearls - NCBI BookshelfDhany karubuyNoch keine Bewertungen
- Low-Intensity Millimeter Waves in Biology and MedicineDokument32 SeitenLow-Intensity Millimeter Waves in Biology and MedicineminunatNoch keine Bewertungen
- Nampath MonositDokument8 SeitenNampath MonositEllya Latifah IlyasNoch keine Bewertungen
- Microbiology An Introduction: Thirteenth EditionDokument47 SeitenMicrobiology An Introduction: Thirteenth EditionAnonymous r0fhYUnuNoch keine Bewertungen
- Non-Specific Host DefensesDokument121 SeitenNon-Specific Host DefensesOmar Christian TuazonNoch keine Bewertungen
- 02 Granulomatous DiseaseDokument141 Seiten02 Granulomatous Diseaseraanja2100% (1)
- Blood and Immunity PowerpointDokument94 SeitenBlood and Immunity Powerpointapi-263357086100% (1)
- Fagocitos Neutrofilos y MonocitosDokument12 SeitenFagocitos Neutrofilos y Monocitoscamilo guerreroNoch keine Bewertungen
- Taxonomic Classification and Pathology of Legionella pneumophilaDokument5 SeitenTaxonomic Classification and Pathology of Legionella pneumophilaOjambo FlaviaNoch keine Bewertungen
- Acute InflammationDokument17 SeitenAcute InflammationMuhammad FaheemNoch keine Bewertungen
- Historical Background and Immune Response OverviewDokument31 SeitenHistorical Background and Immune Response OverviewDiana Rose CallenaNoch keine Bewertungen
- Immunity Basis Diseases 4th EditionDokument88 SeitenImmunity Basis Diseases 4th EditionEdzel Tisado SacloloNoch keine Bewertungen
- Immune Responses: Introduction to Innate and Adaptive ImmunityDokument10 SeitenImmune Responses: Introduction to Innate and Adaptive ImmunityArvi MandaweNoch keine Bewertungen
- CFS Research Long CovidDokument122 SeitenCFS Research Long CovidNikhil BhaskaranNoch keine Bewertungen
- Basic Immunology NotesDokument31 SeitenBasic Immunology NotesKannan MarikaniNoch keine Bewertungen
- Updates On Clinical Trials Evaluating The Regenerative Potential of Allogenic Mesenchymal Stem Cells in COVID-19Dokument11 SeitenUpdates On Clinical Trials Evaluating The Regenerative Potential of Allogenic Mesenchymal Stem Cells in COVID-19diana.alyNoch keine Bewertungen
- CH 22 Lymphatics F 2017Dokument143 SeitenCH 22 Lymphatics F 2017JuliaNoch keine Bewertungen
- MetS genetic links and pathogenesis updateDokument15 SeitenMetS genetic links and pathogenesis updateMunteanu DragosNoch keine Bewertungen
- Mycobacterium Lecture NotesDokument10 SeitenMycobacterium Lecture NotesHansmeet KourNoch keine Bewertungen
- Why Women May Be Better Equipped To Fight COVIDDokument46 SeitenWhy Women May Be Better Equipped To Fight COVIDjudith retanaNoch keine Bewertungen
- Body's Battles (gnv64) PDFDokument96 SeitenBody's Battles (gnv64) PDFameyparanjape100% (1)
- 10 Pharmacology - ImmunopharmacologyDokument17 Seiten10 Pharmacology - ImmunopharmacologyArnoldBorromeoNoch keine Bewertungen