Das könnte Ihnen auch gefallen
- Tennis Elbow - StatPearls - NCBI BookshelfDokument9 SeitenTennis Elbow - StatPearls - NCBI BookshelfADITYA ARI HERLAMBANGNoch keine Bewertungen
- Anatomi Fisiologi KorneaDokument11 SeitenAnatomi Fisiologi KorneaMauVeeNoch keine Bewertungen
- Z Scores GirlsDokument7 SeitenZ Scores GirlsJames Karl HugoNoch keine Bewertungen
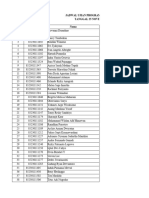
- Jadwal-Ujian-Tpa-Program-Spesialis-Pascasarjana-Sesi-IDokument32 SeitenJadwal-Ujian-Tpa-Program-Spesialis-Pascasarjana-Sesi-IAndrio PalayukanNoch keine Bewertungen
- Rumah Sakit Tk. Iv Samarinda: A. Poliklinik BedahDokument5 SeitenRumah Sakit Tk. Iv Samarinda: A. Poliklinik Bedahhadi sunandarNoch keine Bewertungen
- Dr. I DEWA PUTU SP - PD KGer - TATALAKSANA FARMAKOLOGIK TERBARU HIPERURISEMIA DAN GOUT USIA LANJUTDokument51 SeitenDr. I DEWA PUTU SP - PD KGer - TATALAKSANA FARMAKOLOGIK TERBARU HIPERURISEMIA DAN GOUT USIA LANJUTCOVID RSHJNoch keine Bewertungen
- Group SSDokument19 SeitenGroup SSayang stevenNoch keine Bewertungen
- Kurva Z Score WhoDokument21 SeitenKurva Z Score WhoFenty IswarNoch keine Bewertungen
- Vaginismus A Review of The Literature On The Classification Diagnosis, Etiology and Treatment TranslateDokument14 SeitenVaginismus A Review of The Literature On The Classification Diagnosis, Etiology and Treatment TranslateErliana FaniNoch keine Bewertungen
- Bundle Program Kerja AMSA-Indonesia 20202021 (1) 3Dokument407 SeitenBundle Program Kerja AMSA-Indonesia 20202021 (1) 3Anphauteks LaniaNoch keine Bewertungen
- LP Syok SepsisDokument81 SeitenLP Syok Sepsisrila lagarusuNoch keine Bewertungen
- Glomerular Disease - Evaluation and Differential Diagnosis in Adults - UpToDateDokument23 SeitenGlomerular Disease - Evaluation and Differential Diagnosis in Adults - UpToDateRaiya MallickNoch keine Bewertungen
- PhysioEx Exercise 5 Activity 1Dokument3 SeitenPhysioEx Exercise 5 Activity 1villanuevaparedesaracely4Noch keine Bewertungen
- Stroke Hemoragic: Sebagai Salah Satu Tugas Mata Kuliah TIK Akademi Keperawatan (Akper) SawerigadingDokument10 SeitenStroke Hemoragic: Sebagai Salah Satu Tugas Mata Kuliah TIK Akademi Keperawatan (Akper) SawerigadingMade Serly KrisdayantiNoch keine Bewertungen
- General Principles of Cell OrganisationDokument3 SeitenGeneral Principles of Cell Organisation22194Noch keine Bewertungen
- Kelompok: Obat Kategori: Generik (E-Katalog) : Penawaran Harga Kimia FarmaDokument15 SeitenKelompok: Obat Kategori: Generik (E-Katalog) : Penawaran Harga Kimia FarmaGudang ObatNoch keine Bewertungen
- Medel SonataDokument54 SeitenMedel Sonatamaclab macNoch keine Bewertungen
- Tenses: Exercise 48: Translate Into Good English!Dokument92 SeitenTenses: Exercise 48: Translate Into Good English!haygia andari27Noch keine Bewertungen
- Six Building Blocks Dan Health SystemDokument6 SeitenSix Building Blocks Dan Health SystemDiar DiarNoch keine Bewertungen
- Jurnal Bahasa InggrisDokument7 SeitenJurnal Bahasa Inggrisimma lholhypopNoch keine Bewertungen
- Makalah Inggris SalwaDokument18 SeitenMakalah Inggris Salwawatashiwa kyraNoch keine Bewertungen
- 2.heart Rate - An Emerging Risk Factor in CVDDokument49 Seiten2.heart Rate - An Emerging Risk Factor in CVDAkhil SharmaNoch keine Bewertungen
- Kecemasan Pada Lansia PDFDokument7 SeitenKecemasan Pada Lansia PDFJoecoNoch keine Bewertungen
- Weight-for-Height GIRLS: 2 To 5 Years (Z-Scores)Dokument1 SeiteWeight-for-Height GIRLS: 2 To 5 Years (Z-Scores)Malisa LukmanNoch keine Bewertungen
- Stunting 2022Dokument2 SeitenStunting 2022HASTA MUNANoch keine Bewertungen
- What Do We Know About Patent Dustus Arteriosus - Dr. Adhi Teguh, Sp.a (K)Dokument39 SeitenWhat Do We Know About Patent Dustus Arteriosus - Dr. Adhi Teguh, Sp.a (K)laurentiaNoch keine Bewertungen
- Perbandingan Metode Klamp Dan Lem Terhadap Penyembuhan Luka Pasca Sirkumsisi Pada AnakDokument6 SeitenPerbandingan Metode Klamp Dan Lem Terhadap Penyembuhan Luka Pasca Sirkumsisi Pada Anaknanang prasetyoNoch keine Bewertungen
- Correlation Between Body Mass Index and Intraocular Pressure at Eye Clinic Mangusada Hospital, BaliDokument3 SeitenCorrelation Between Body Mass Index and Intraocular Pressure at Eye Clinic Mangusada Hospital, BaliKarina NathaniaNoch keine Bewertungen
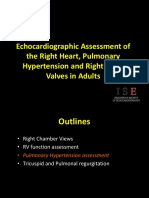
- 3 - Right Heart AssessmentDokument47 Seiten3 - Right Heart Assessmentpatricia wageyNoch keine Bewertungen
- SR Prodia 2021 FinalDokument96 SeitenSR Prodia 2021 FinalJavarion AidenNoch keine Bewertungen
- Dapsa EngDokument1 SeiteDapsa EngwawanpecelNoch keine Bewertungen
- Factors Affecting The Use of Quick Response Code Indonesian Standard (QRIS) With The Unified Theory of Acceptance and Use of Technology ModelDokument6 SeitenFactors Affecting The Use of Quick Response Code Indonesian Standard (QRIS) With The Unified Theory of Acceptance and Use of Technology ModelInternational Journal of Innovative Science and Research TechnologyNoch keine Bewertungen
- LP Thalasemia - YETTIDokument12 SeitenLP Thalasemia - YETTIYetty MalauNoch keine Bewertungen
- Proliferasi SelDokument50 SeitenProliferasi SelIkan SeluangNoch keine Bewertungen
- Stenosis RenalisDokument21 SeitenStenosis Renalismargharita komboyNoch keine Bewertungen
- Tugas Contoh EKG KucingDokument3 SeitenTugas Contoh EKG KucingalfiyanNoch keine Bewertungen
- Metals As Co-Enzymes and Their SignificanceDokument10 SeitenMetals As Co-Enzymes and Their Significanceom prakash royNoch keine Bewertungen
- Pamflet - Symposium & Workshop Spiritual and Religious Psychiatry Update 31 Agustus 2022Dokument5 SeitenPamflet - Symposium & Workshop Spiritual and Religious Psychiatry Update 31 Agustus 2022Immas Wahyu FajariniNoch keine Bewertungen
- Hubungan Pengetahuan Tentang Hipertensi, Asupan Lemak Dan Natrium Dengan Status Gizi Di Posyandu Lansia, Gonilan, Kartasura, SukoharjoDokument20 SeitenHubungan Pengetahuan Tentang Hipertensi, Asupan Lemak Dan Natrium Dengan Status Gizi Di Posyandu Lansia, Gonilan, Kartasura, SukoharjoDinaNoch keine Bewertungen
- Skripsi Tanpa Bab Pembahasan PDFDokument53 SeitenSkripsi Tanpa Bab Pembahasan PDFRini Aprianti PurbaNoch keine Bewertungen
- Kelainan Pada Sistem Saraf PeriferDokument144 SeitenKelainan Pada Sistem Saraf PeriferArtika MayandaNoch keine Bewertungen
- LP CHFDokument14 SeitenLP CHFPutra Nova PrasetiaNoch keine Bewertungen
- Jadwal Acara PIT POGI 25 Padang Update 3 Sept 2021Dokument8 SeitenJadwal Acara PIT POGI 25 Padang Update 3 Sept 2021daniel_alexander_susenoNoch keine Bewertungen
- Ukt Kel 1 2022Dokument40 SeitenUkt Kel 1 2022Wulan NurniantyNoch keine Bewertungen
- Persistent and Chronic Diarrhea and Malabsorption - ESPGHAN PDFDokument6 SeitenPersistent and Chronic Diarrhea and Malabsorption - ESPGHAN PDFMoises RiveraNoch keine Bewertungen
- Skripsi Tanpa Bab Pembahasan PDFDokument67 SeitenSkripsi Tanpa Bab Pembahasan PDFaaaaNoch keine Bewertungen
- Name: Cauilan, Darwin C. Score: Year and Section: Bs Pharma 1-A Set A DateDokument4 SeitenName: Cauilan, Darwin C. Score: Year and Section: Bs Pharma 1-A Set A DateDarwin CauilanNoch keine Bewertungen
- Summary NotesDokument11 SeitenSummary NotessamNoch keine Bewertungen
- Ch12 OL SummaryDokument47 SeitenCh12 OL Summaryzuhra123coolNoch keine Bewertungen
- Assignment Lec 4Dokument3 SeitenAssignment Lec 4morriganNoch keine Bewertungen
- Peripheral Nervous SystemDokument7 SeitenPeripheral Nervous SystemAhmad Althof Malihul AdiNoch keine Bewertungen
- What Is A Neuron Diagrams, Types, Function, and More PDFDokument1 SeiteWhat Is A Neuron Diagrams, Types, Function, and More PDFSantiago BarbosaNoch keine Bewertungen
- Group 9 Neuron Structure & FunctionDokument14 SeitenGroup 9 Neuron Structure & FunctionMosesNoch keine Bewertungen
- Notes-2 NPDokument7 SeitenNotes-2 NPPranavi KhandekarNoch keine Bewertungen
- NeuronsDokument24 SeitenNeuronsKen Ross ManansalaNoch keine Bewertungen
- Nervous CommunicationDokument13 SeitenNervous CommunicationWang PengfeiNoch keine Bewertungen
- Control and CoordiantionDokument25 SeitenControl and CoordiantionnoNoch keine Bewertungen
- Nervous Coordination and ResponseDokument11 SeitenNervous Coordination and ResponseJashya NoorNoch keine Bewertungen
- NervoussystemlabreportDokument9 SeitenNervoussystemlabreportapi-296594736Noch keine Bewertungen
- 1 SEMESTER 18/19: Median Nerve-Carpal Tunnel Weakens Lateral 3 Digits Sensory Loss ParalysisDokument60 Seiten1 SEMESTER 18/19: Median Nerve-Carpal Tunnel Weakens Lateral 3 Digits Sensory Loss ParalysisInsaf AhamedNoch keine Bewertungen
- Inner SmileDokument1 SeiteInner SmileIon ConstantinNoch keine Bewertungen
- Lumbar DiscopathyDokument3 SeitenLumbar DiscopathyPirasan Traditional Medicine CenterNoch keine Bewertungen
- Teeth Science Year 3 (Milk and Permanent) ActivityDokument10 SeitenTeeth Science Year 3 (Milk and Permanent) ActivityVaishnavi KrishnanNoch keine Bewertungen
- HAP Question Bank Sem 2 B PharmDokument4 SeitenHAP Question Bank Sem 2 B PharmJeswin AntoNoch keine Bewertungen
- AFAA Personal Trainer CertificationDokument7 SeitenAFAA Personal Trainer CertificationubersteveNoch keine Bewertungen
- Lumbar Disc Herniation: Prof - Dr.Hidayet Sarı Physical Medicine and Rehabilitation DepartmentDokument20 SeitenLumbar Disc Herniation: Prof - Dr.Hidayet Sarı Physical Medicine and Rehabilitation DepartmentraraNoch keine Bewertungen
- Brachial Plexus InjuriesDokument345 SeitenBrachial Plexus Injuriesmohamedwhatever100% (2)
- Anatomy-Physiology of ThyroidDokument10 SeitenAnatomy-Physiology of ThyroidnabillaoktaviaNoch keine Bewertungen
- 100 Diseases Treated by Single Point of AcupunctureDokument209 Seiten100 Diseases Treated by Single Point of AcupunctureAgeng Rikhmawan100% (31)
- Lumbar Spine SampleDokument3 SeitenLumbar Spine SampleRizky NoviantoroNoch keine Bewertungen
- Cardiac Anatomy Using CTDokument39 SeitenCardiac Anatomy Using CTDyah KumalasariNoch keine Bewertungen
- ICSE Skin WorksheetDokument1 SeiteICSE Skin WorksheetpreetaNoch keine Bewertungen
- Core Training EvidenceDokument14 SeitenCore Training EvidenceKarol MachadoNoch keine Bewertungen
- Vascular Trauma, Dies Natalis FK UHDokument31 SeitenVascular Trauma, Dies Natalis FK UHJayarasti KusumanegaraNoch keine Bewertungen
- Anatomy SpleenDokument32 SeitenAnatomy SpleenBijo K BennyNoch keine Bewertungen
- Deltoid Re-Education Program For Massive Rotator Cuff Tears: Ofer Levy, MD, MCH (Orth), FrcsDokument12 SeitenDeltoid Re-Education Program For Massive Rotator Cuff Tears: Ofer Levy, MD, MCH (Orth), FrcsDavid DizonNoch keine Bewertungen
- Final Internalmed2Dokument1.788 SeitenFinal Internalmed2Sharayu DhobleNoch keine Bewertungen
- Difficult Airway AlgorithmDokument48 SeitenDifficult Airway AlgorithmshikhaNoch keine Bewertungen
- Guidelines For Basic Adult Neurological Observation: Neurosurgical Nurse Educator NetworkDokument20 SeitenGuidelines For Basic Adult Neurological Observation: Neurosurgical Nurse Educator NetworkSimon S. KledenNoch keine Bewertungen
- Efecto de La Presión en La Filtración GlomerularDokument4 SeitenEfecto de La Presión en La Filtración GlomerularLuisitaMariaNoch keine Bewertungen
- Lesson17 Epithelial CellsDokument22 SeitenLesson17 Epithelial CellsGemma WrigleyNoch keine Bewertungen
- The Naming of The Cranial Nerves - A Historical ReviewDokument7 SeitenThe Naming of The Cranial Nerves - A Historical ReviewAfnan SefffNoch keine Bewertungen
- Tarsal Tunnel SyndromeDokument21 SeitenTarsal Tunnel SyndromedrarunraoNoch keine Bewertungen
- Thyroid Disorders: Dr. Lubna DwerijDokument52 SeitenThyroid Disorders: Dr. Lubna DwerijNoor MajaliNoch keine Bewertungen
- CirculationDokument10 SeitenCirculationMohd Azrul DsevenNoch keine Bewertungen
- GORUCK Heavy - WEEK 1 PDFDokument1 SeiteGORUCK Heavy - WEEK 1 PDFJohn RohrerNoch keine Bewertungen
- Aecep Fascia1Dokument21 SeitenAecep Fascia1Luis Fernando Ruiz Esparza AguileraNoch keine Bewertungen
- Body CordinationDokument13 SeitenBody CordinationmaryamsyuhadaNoch keine Bewertungen
- The SpineDokument422 SeitenThe Spinedayane2394100% (2)