Das könnte Ihnen auch gefallen
- Cognitive and Behavioral Interventions in the Schools: Integrating Theory and Research into PracticeVon EverandCognitive and Behavioral Interventions in the Schools: Integrating Theory and Research into PracticeRosemary FlanaganNoch keine Bewertungen
- Acrofobia 5Dokument4 SeitenAcrofobia 5Teinei :vNoch keine Bewertungen
- Psychiatric Diagnosis: Challenges and ProspectsVon EverandPsychiatric Diagnosis: Challenges and ProspectsIhsan M. SalloumBewertung: 5 von 5 Sternen5/5 (1)
- Comparison of Self-Report and Overt-Behavioral Procedures For Assessing AcrophobiaDokument7 SeitenComparison of Self-Report and Overt-Behavioral Procedures For Assessing AcrophobiaMiztaloges86Noch keine Bewertungen
- Young's Schema Questionnaire - Short Form Version 3 (YSQ-S3) : Preliminary Validation in Older AdultsDokument35 SeitenYoung's Schema Questionnaire - Short Form Version 3 (YSQ-S3) : Preliminary Validation in Older AdultsFiona DayNoch keine Bewertungen
- Psychology AssignmentDokument7 SeitenPsychology AssignmentnaveedNoch keine Bewertungen
- (Hollon, 2010) - The Cognitive RevolutionDokument12 Seiten(Hollon, 2010) - The Cognitive RevolutionEileen GarcíaNoch keine Bewertungen
- The Littering Attitude Scale PDFDokument15 SeitenThe Littering Attitude Scale PDFAnonymous jvb1l3huqbNoch keine Bewertungen
- Dummy ReportDokument29 SeitenDummy ReportnaquiahoNoch keine Bewertungen
- The Autism Observation Scale For Infants: Scale Development and Reliability DataDokument8 SeitenThe Autism Observation Scale For Infants: Scale Development and Reliability DataRenata de Mesquita Ferraz LucenaNoch keine Bewertungen
- JoDD 17-1 26-37 Schroeder Et AlDokument12 SeitenJoDD 17-1 26-37 Schroeder Et AlEspíritu CiudadanoNoch keine Bewertungen
- Eysenck Personality To CommunicateDokument48 SeitenEysenck Personality To CommunicateYenni RoeshintaNoch keine Bewertungen
- Module 1 CBTDokument9 SeitenModule 1 CBTJasroop MahalNoch keine Bewertungen
- 1968 - Kiresuk, T. Sherman, R.Dokument11 Seiten1968 - Kiresuk, T. Sherman, R.nataliacnNoch keine Bewertungen
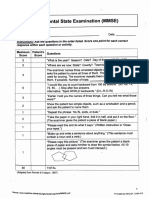
- Mini-Mental State Examination (MMSE)Dokument3 SeitenMini-Mental State Examination (MMSE)Prescilla San PedroNoch keine Bewertungen
- A Brief History of The Origins of Behavioral MedicineDokument16 SeitenA Brief History of The Origins of Behavioral MedicineAllie WatrenNoch keine Bewertungen
- Adolescents Choosing Self-Harm As An Emotion RegulationDokument14 SeitenAdolescents Choosing Self-Harm As An Emotion RegulationmiriamNoch keine Bewertungen
- Riverside YAT Program LawsuitDokument70 SeitenRiverside YAT Program LawsuitFindLawNoch keine Bewertungen
- CatDokument12 SeitenCatnini345Noch keine Bewertungen
- Take The Quiz: Please Note: This Test Will Only Be Scored Correctly If You Answer Each One of TheDokument4 SeitenTake The Quiz: Please Note: This Test Will Only Be Scored Correctly If You Answer Each One of TheAriane VidalNoch keine Bewertungen
- Zaki & Williams (2013) - Interpersonal Emotion RegulationDokument9 SeitenZaki & Williams (2013) - Interpersonal Emotion Regulationalessarpon7557Noch keine Bewertungen
- OARS Adl IadlDokument5 SeitenOARS Adl IadlSamuelNoch keine Bewertungen
- Csep-II Experiential Therapy Session FormDokument16 SeitenCsep-II Experiential Therapy Session FormSicologo Felipe PuertaNoch keine Bewertungen
- Covid-19 Pandemic Mental Health Questionnaire (Copaq)Dokument9 SeitenCovid-19 Pandemic Mental Health Questionnaire (Copaq)JeleneNoch keine Bewertungen
- Negative Symptoms EQZ Lancet ReviewDokument14 SeitenNegative Symptoms EQZ Lancet ReviewConstanza González GutiérrezNoch keine Bewertungen
- Lo3 Artifact - Micro-Counseling Skills Midterm ReflectionDokument6 SeitenLo3 Artifact - Micro-Counseling Skills Midterm Reflectionapi-543749170Noch keine Bewertungen
- Subtest OriginsDokument38 SeitenSubtest OriginsCharlie HultgreenNoch keine Bewertungen
- Conflicte NormeDokument18 SeitenConflicte Normekoakaze100% (1)
- The Co-Occurrence of Intellectual Giftedness and Autism Spectrum 2011Dokument22 SeitenThe Co-Occurrence of Intellectual Giftedness and Autism Spectrum 2011Ingrid DíazNoch keine Bewertungen
- The Empty ChairDokument1 SeiteThe Empty Chairapi-244827434Noch keine Bewertungen
- Fmri and PsychologyDokument14 SeitenFmri and Psychologyapi-478952871Noch keine Bewertungen
- CV For Dr. Keely KolmesDokument9 SeitenCV For Dr. Keely KolmesdrkkolmesNoch keine Bewertungen
- Clinician Tabel Skizofrenia DSM VDokument4 SeitenClinician Tabel Skizofrenia DSM VrayendrarenoNoch keine Bewertungen
- QS: Social Exchange Theory: FoundersDokument2 SeitenQS: Social Exchange Theory: FounderssoulxpressNoch keine Bewertungen
- Therapy in Action Psychoanalytic TherapyDokument23 SeitenTherapy in Action Psychoanalytic TherapyIoana Voina100% (1)
- Manual SiqDokument4 SeitenManual SiqumieNoch keine Bewertungen
- 1999 Aversion Therapy-BEDokument6 Seiten1999 Aversion Therapy-BEprabhaNoch keine Bewertungen
- SDQDokument3 SeitenSDQSarah AzminNoch keine Bewertungen
- Frontal Lobe SyndromeDokument67 SeitenFrontal Lobe SyndromeVIJAYKUMAR HIREMATH100% (1)
- A Reliability and Validity Study of The State-Trait Anxiety InventoryDokument5 SeitenA Reliability and Validity Study of The State-Trait Anxiety InventoryYilin NgNoch keine Bewertungen
- The Thurstone Temperament Schedule As An Instrument of SupervisorDokument72 SeitenThe Thurstone Temperament Schedule As An Instrument of Supervisoracordero0% (1)
- Scales For BIpolar DisorderDokument14 SeitenScales For BIpolar DisorderDivia RainaNoch keine Bewertungen
- DSM 5 (ASD - Guidelines) Feb2013Dokument7 SeitenDSM 5 (ASD - Guidelines) Feb2013Marubare CárdenasNoch keine Bewertungen
- Oxford Handbooks Online: Intellectual DisabilitiesDokument20 SeitenOxford Handbooks Online: Intellectual DisabilitiesCristina100% (1)
- Group Therapy PDFDokument2 SeitenGroup Therapy PDFma maNoch keine Bewertungen
- Emotional Intelligence and The Trait Meta-Mood ScaleDokument13 SeitenEmotional Intelligence and The Trait Meta-Mood Scalediego polinarioNoch keine Bewertungen
- Tolman Theory of LearningDokument4 SeitenTolman Theory of LearningBigyan BasaulaNoch keine Bewertungen
- Detection of Bipolar Disorder BJP 2011 Young 3 4Dokument3 SeitenDetection of Bipolar Disorder BJP 2011 Young 3 4Gede GiriNoch keine Bewertungen
- Clinician Tabel Skizofrenia DSM VDokument2 SeitenClinician Tabel Skizofrenia DSM VAndriati NadhilaNoch keine Bewertungen
- Functionalism: American Psychology Takes HoldDokument17 SeitenFunctionalism: American Psychology Takes HoldTehran DavisNoch keine Bewertungen
- Questionnaire DAR 5 Dimensions of Anger ReactionsDokument2 SeitenQuestionnaire DAR 5 Dimensions of Anger ReactionsJerome Jiro Rada HerminigildoNoch keine Bewertungen
- Teenage AnxietyDokument34 SeitenTeenage Anxietyamit100% (1)
- 1983 - The Brief Symptom Inventory, An Introductory ReportDokument11 Seiten1983 - The Brief Symptom Inventory, An Introductory ReportBogdan BaceanuNoch keine Bewertungen
- Strasburger Et Al-2015-PsyCh JournalDokument8 SeitenStrasburger Et Al-2015-PsyCh JournalPedro CardosoNoch keine Bewertungen
- Handouts YBOC Symptom ChecklistDokument2 SeitenHandouts YBOC Symptom ChecklistJoem cNoch keine Bewertungen
- Down's Syndrome Pada KehamilanDokument35 SeitenDown's Syndrome Pada KehamilanArga AdityaNoch keine Bewertungen
- Zuber-Skerritt-New Directions in Action Research (1996) PDFDokument234 SeitenZuber-Skerritt-New Directions in Action Research (1996) PDFbeatrixNoch keine Bewertungen
- Intelligence and Emotional Disorders - PAID - 2015 PDFDokument4 SeitenIntelligence and Emotional Disorders - PAID - 2015 PDFOmar Azaña Velez100% (1)
- Y Bocs Information SampleDokument2 SeitenY Bocs Information SampledevNoch keine Bewertungen
- Bol Practical Research 1 and 2Dokument2 SeitenBol Practical Research 1 and 2ggonegvftNoch keine Bewertungen
- Motivation, Health-Related Lifestyles and Depression Among University StudentsDokument6 SeitenMotivation, Health-Related Lifestyles and Depression Among University StudentsLina SantosNoch keine Bewertungen
- A Study On Employee Welfare Measure at Vimpro Tech PuducherryDokument3 SeitenA Study On Employee Welfare Measure at Vimpro Tech PuducherryEditor IJTSRDNoch keine Bewertungen
- Hanna MulugetaDokument150 SeitenHanna MulugetaKidu YabeNoch keine Bewertungen
- Statistics NotesDokument18 SeitenStatistics Notesmike chanNoch keine Bewertungen
- Practical Guide To Auditing The Software Development ProcessDokument17 SeitenPractical Guide To Auditing The Software Development ProcessBruno Collet100% (5)
- Exercise 1:: Chapter 3: Describing Data: Numerical MeasuresDokument11 SeitenExercise 1:: Chapter 3: Describing Data: Numerical MeasuresPW Nicholas100% (1)
- A Synopsis Report ON "Performance Appraisal" AT "Rks Motors Pvt. LTD" Submitted By: K.N.Bindu Bhargavi (118917672026)Dokument8 SeitenA Synopsis Report ON "Performance Appraisal" AT "Rks Motors Pvt. LTD" Submitted By: K.N.Bindu Bhargavi (118917672026)Swaneeth SheelNoch keine Bewertungen
- D4524-86 (Reapproved 2012) PDFDokument4 SeitenD4524-86 (Reapproved 2012) PDFakbarNoch keine Bewertungen
- Literature Review Seating ArrangementDokument7 SeitenLiterature Review Seating Arrangementfat1kifywel3100% (1)
- BL-RSCH-2122-LEC-1922S Inquiries, Investigations and ImmersionDokument76 SeitenBL-RSCH-2122-LEC-1922S Inquiries, Investigations and ImmersionJane Sandoval100% (1)
- Als Chapter 3Dokument4 SeitenAls Chapter 3cj azucena100% (1)
- Assignment 2Dokument22 SeitenAssignment 2Nurul Absar RashedNoch keine Bewertungen
- LEO Group 7Dokument21 SeitenLEO Group 7Mariecriz Balaba BanaezNoch keine Bewertungen
- As 9102 FaiDokument3 SeitenAs 9102 FaiKarthi ThiyagarajanNoch keine Bewertungen
- Edited - Capstone Project Proposal Draft Student Fillable 1Dokument6 SeitenEdited - Capstone Project Proposal Draft Student Fillable 1api-615322707Noch keine Bewertungen
- Credo NCSS3 ReportDokument81 SeitenCredo NCSS3 ReportFaze amuzante '16Noch keine Bewertungen
- TABLE Front PageDokument10 SeitenTABLE Front PagevkNoch keine Bewertungen
- Calibration and Quality Control in The LaboratoryDokument15 SeitenCalibration and Quality Control in The LaboratoryChrisarh NofuenteNoch keine Bewertungen
- Body Wash Case StudyDokument6 SeitenBody Wash Case StudyFebin KoyanNoch keine Bewertungen
- Assessing The Causes & Impacts of Traffic Congestion On The Society, Economy and Individual: A Case of Mauritius As An Emerging EconomyDokument13 SeitenAssessing The Causes & Impacts of Traffic Congestion On The Society, Economy and Individual: A Case of Mauritius As An Emerging EconomyJohn Lloyd BallaNoch keine Bewertungen
- Omkar Katkar - Final Draft - Marketing - B88Dokument73 SeitenOmkar Katkar - Final Draft - Marketing - B88Nisha AgrawalNoch keine Bewertungen
- Why Interview?: 8 Interviewing As Qualitative ResearchDokument4 SeitenWhy Interview?: 8 Interviewing As Qualitative ResearchfarumasNoch keine Bewertungen
- Background of Tourism in BangladeshDokument8 SeitenBackground of Tourism in BangladeshNudrat ZaheenNoch keine Bewertungen
- Naval Postgraduate School: Monterey, CaliforniaDokument107 SeitenNaval Postgraduate School: Monterey, CaliforniascriiNoch keine Bewertungen
- An Introduction To Quantitative ResearchDokument5 SeitenAn Introduction To Quantitative ResearchShradha NambiarNoch keine Bewertungen
- Project Management Dissertation Topics PDFDokument6 SeitenProject Management Dissertation Topics PDFBuyCheapPaperOnlineScottsdale100% (1)
- Winsorized Modified One Step M-Estimator As A Measure of The Central Tendency in The Alexander-Govern TestDokument13 SeitenWinsorized Modified One Step M-Estimator As A Measure of The Central Tendency in The Alexander-Govern Test23222048Noch keine Bewertungen
- Artikel1 PerancanganDokument10 SeitenArtikel1 PerancanganPalaganesh NaiduNoch keine Bewertungen
- Acc 35 PDFDokument10 SeitenAcc 35 PDFrifkiNoch keine Bewertungen
- Love Life: How to Raise Your Standards, Find Your Person, and Live Happily (No Matter What)Von EverandLove Life: How to Raise Your Standards, Find Your Person, and Live Happily (No Matter What)Bewertung: 3 von 5 Sternen3/5 (1)
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionVon EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionBewertung: 4 von 5 Sternen4/5 (404)
- By the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsVon EverandBy the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsNoch keine Bewertungen
- The Age of Magical Overthinking: Notes on Modern IrrationalityVon EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityBewertung: 4 von 5 Sternen4/5 (32)
- Summary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisVon EverandSummary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisBewertung: 4.5 von 5 Sternen4.5/5 (42)
- ADHD is Awesome: A Guide to (Mostly) Thriving with ADHDVon EverandADHD is Awesome: A Guide to (Mostly) Thriving with ADHDBewertung: 5 von 5 Sternen5/5 (3)
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeVon EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeBewertung: 2 von 5 Sternen2/5 (1)
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedVon EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedBewertung: 4.5 von 5 Sternen4.5/5 (82)
- Cult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryVon EverandCult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryBewertung: 4 von 5 Sternen4/5 (46)
- The Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaVon EverandThe Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- The Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsVon EverandThe Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsBewertung: 4 von 5 Sternen4/5 (4)
- The Obesity Code: Unlocking the Secrets of Weight LossVon EverandThe Obesity Code: Unlocking the Secrets of Weight LossBewertung: 4 von 5 Sternen4/5 (6)
- Manipulation: The Ultimate Guide To Influence People with Persuasion, Mind Control and NLP With Highly Effective Manipulation TechniquesVon EverandManipulation: The Ultimate Guide To Influence People with Persuasion, Mind Control and NLP With Highly Effective Manipulation TechniquesBewertung: 4.5 von 5 Sternen4.5/5 (1412)
- Raising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsVon EverandRaising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsBewertung: 5 von 5 Sternen5/5 (1)
- The Comfort of Crows: A Backyard YearVon EverandThe Comfort of Crows: A Backyard YearBewertung: 4.5 von 5 Sternen4.5/5 (23)
- Dark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Von EverandDark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Bewertung: 4.5 von 5 Sternen4.5/5 (110)
- Why We Die: The New Science of Aging and the Quest for ImmortalityVon EverandWhy We Die: The New Science of Aging and the Quest for ImmortalityBewertung: 4 von 5 Sternen4/5 (5)
- Raising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsVon EverandRaising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsBewertung: 4.5 von 5 Sternen4.5/5 (170)
- Summary: Limitless: Upgrade Your Brain, Learn Anything Faster, and Unlock Your Exceptional Life By Jim Kwik: Key Takeaways, Summary and AnalysisVon EverandSummary: Limitless: Upgrade Your Brain, Learn Anything Faster, and Unlock Your Exceptional Life By Jim Kwik: Key Takeaways, Summary and AnalysisBewertung: 5 von 5 Sternen5/5 (8)
- When the Body Says No by Gabor Maté: Key Takeaways, Summary & AnalysisVon EverandWhen the Body Says No by Gabor Maté: Key Takeaways, Summary & AnalysisBewertung: 3.5 von 5 Sternen3.5/5 (2)
- Mindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessVon EverandMindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessBewertung: 4.5 von 5 Sternen4.5/5 (328)
- Troubled: A Memoir of Foster Care, Family, and Social ClassVon EverandTroubled: A Memoir of Foster Care, Family, and Social ClassBewertung: 4.5 von 5 Sternen4.5/5 (27)
- Dark Psychology: Learn To Influence Anyone Using Mind Control, Manipulation And Deception With Secret Techniques Of Dark Persuasion, Undetected Mind Control, Mind Games, Hypnotism And BrainwashingVon EverandDark Psychology: Learn To Influence Anyone Using Mind Control, Manipulation And Deception With Secret Techniques Of Dark Persuasion, Undetected Mind Control, Mind Games, Hypnotism And BrainwashingBewertung: 4 von 5 Sternen4/5 (1138)
- The Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeVon EverandThe Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeBewertung: 4.5 von 5 Sternen4.5/5 (254)