Beruflich Dokumente
Kultur Dokumente
Choice, Transparency, Coordination, and Quality Among Direct-to-Consumer Telemedicine Websites and Apps Treating Skin Disease
Hochgeladen von
MikeOriginaltitel
Copyright
Verfügbare Formate
Dieses Dokument teilen
Dokument teilen oder einbetten
Stufen Sie dieses Dokument als nützlich ein?
Sind diese Inhalte unangemessen?
Dieses Dokument meldenCopyright:
Verfügbare Formate
Choice, Transparency, Coordination, and Quality Among Direct-to-Consumer Telemedicine Websites and Apps Treating Skin Disease
Hochgeladen von
MikeCopyright:
Verfügbare Formate
Research
Original Investigation
Choice, Transparency, Coordination, and Quality Among
Direct-to-Consumer Telemedicine Websites
and Apps Treating Skin Disease
Jack S. Resneck Jr, MD; Michael Abrouk; Meredith Steuer, MMS; Andrew Tam; Adam Yen; Ivy Lee, MD;
Carrie L. Kovarik, MD; Karen E. Edison, MD
Editor's Note
IMPORTANCE Evidence supports use of teleconsultation for improving patient access to
dermatology. However, little is known about the quality of rapidly expanding
direct-to-consumer (DTC) telemedicine websites and smartphone apps diagnosing and
treating skin disease.
OBJECTIVE To assess the performance of DTC teledermatology services.
DESIGN AND PARTICIPANTS Simulated patients submitted a series of structured dermatologic
cases with photographs, including neoplastic, inflammatory, and infectious conditions, using
regional and national DTC telemedicine websites and smartphone apps offering services to
California residents.
MAIN OUTCOMES AND MEASURES Choice of clinician, transparency of credentials, clinician
location, demographic and medical data requested, diagnoses given, treatments
recommended or prescribed, adverse effects discussed, care coordination.
RESULTS We received responses for 62 clinical encounters from 16 DTC telemedicine
websites from February 4 to March 11, 2016. None asked for identification or raised concerns
about pseudonym use or falsified photographs. During most encounters (42 [68%]), patients
were assigned a clinician without any choice. Only 16 (26%) disclosed information about
clinician licensure, and some used internationally based physicians without California
licenses. Few collected the name of an existing primary care physician (14 [23%]) or offered
to send records (6 [10%]). A diagnosis or likely diagnosis was proffered in 48 encounters
(77%). Prescription medications were ordered in 31 of 48 diagnosed cases (65%), and
relevant adverse effects or pregnancy risks were disclosed in a minority (10 of 31 [32%] and
6 of 14 [43%], respectively). Websites made several correct diagnoses in clinical scenarios
where photographs alone were adequate, but when basic additional history elements (eg,
fever, hypertrichosis, oligomenorrhea) were important, they regularly failed to ask simple
relevant questions and diagnostic performance was poor. Major diagnoses were repeatedly
missed, including secondary syphilis, eczema herpeticum, gram-negative folliculitis, and
Author Affiliations: Department of
polycystic ovarian syndrome. Regardless of the diagnoses given, treatments prescribed were Dermatology, and Philip R. Lee
sometimes at odds with existing guidelines. Institute for Health Policy Studies,
University of California, San Francisco
School of Medicine, San Francisco
CONCLUSIONS AND RELEVANCE Telemedicine has potential to expand access to high-value (Resneck); University of California,
health care. Our findings, however, raise concerns about the quality of skin disease diagnosis San Francisco School of Medicine,
and treatment provided by many DTC telemedicine websites. Ongoing expansion of health San Francisco (Abrouk, Steuer, Tam,
Yen); Pasadena Premier Dermatology,
plan coverage of these services may be premature. Until improvements are made, patients
Pasadena, California (Lee);
risk using health care services that lack transparency, choice, thoroughness, diagnostic and Department of Dermatology,
therapeutic quality, and care coordination. We offer several suggestions to improve the University of Pennsylvania,
quality of DTC telemedicine websites and apps and avoid further growth of fragmented, Philadelphia (Kovarik); Department
of Dermatology, University of
low-quality care.
Missouri, Columbia (Edison).
Corresponding Author: Jack S.
Resneck Jr, MD, Department of
Dermatology, University of California,
San Francisco, Box 0316,
JAMA Dermatol. doi:10.1001/jamadermatol.2016.1774 San Francisco, CA 94143-0316
Published online May 15, 2016. (resneckj@derm.ucsf.edu).
(Reprinted) E1
Copyright 2016 American Medical Association. All rights reserved.
Downloaded From: http://archderm.jamanetwork.com/ by a UCSF LIBRARY User on 05/15/2016
Research Original Investigation Direct-to-Consumer Telemedicine Websites Treating Skin Disease
D
ermatology was an early adopter of telemedicine tech-
nologies, and a substantial evidence base has demon- Key Points
strated diagnostic concordance,1-3 improved cost,4 and
Question Are rapidly expanding direct-to-consumer (DTC)
similar outcomes to in-person care5,6 for certain clinical sce- telemedicine websites and apps providing high-quality diagnosis
narios. These positive findings are primarily from store- and treatment for skin diseases?
and-forward (asynchronous) teleconsultation models, where
Findings Sixty-two simulated encounters to 16 DTC telemedicine
a referring clinician sends a patient’s history and images to a
websites resulted in care that often lacked patient choice of
dermatologist for recommendations. clinician, transparency of clinician credentials, or care
Direct-to-consumer (DTC) teledermatology, while less coordination. Many incorrect diagnoses were proffered without
studied, is expanding rapidly. Direct-to-consumer telemedi- reasonable attempts to ask basic medical history follow-up
cine companies have raised substantial investor capital7 and questions, treatment recommendations sometimes contradicted
marketed themselves heavily to consumers, employers, and evidence-based guidelines, and prescriptions frequently lacked
disclosure of possible adverse effects and pregnancy risks.
health plans. Many additional DTC telemedicine websites with
a narrower focus on dermatology have also emerged. While Meaning Telemedicine has potential to expand access, but these
most initially relied on fees paid by individual patients who findings raise doubts about the quality of skin disease diagnosis
sought convenience or inexpensive care, large DTC services are and treatment currently being provided by DTC telemedicine
websites and apps.
increasingly contracting with major health plans to provide
telecare to millions of enrollees.8 Meanwhile, many of these
payers still exclude asynchronous telemedicine services pro- actions with clinicians, each universally submitted HPI (what a
vided by a patient’s existing health care team. patient might think is relevant) was supplemented with additional
While the number of DTC telemedicine website visits in HPI and ROS data that each patient would offer if asked or if there
2015 reached 1.25 million,9 relatively little is known about the was any place in the submission process to include it. The high-
quality of these services. A recent study assessing DTC tele- lights of each case are summarized in Table 1.
medicine consultations for primary care conditions revealed Study personnel accessed each website and app between
a lack of appropriate diagnostic testing and poor antibiotic February 4 and March 11, 2016, posing as patients (all cases were
stewardship.10 Reviews of teledermatology services showed separately submitted to each website, except that acne-only
failures to collect key medical history11 and raised concerns websites received just 2 cases). Study personnel claimed to be
about use of international physicians and advertising promi- uninsured and paid fees using Visa gift debit cards in the names
nently featuring easily obtained prescriptions.12 of the simulated patients. No study personnel provided any
National physician groups, many of which support expanded false government-issued identification cards or numbers. When
telemedicine, have questioned whether these companies are giv- given a choice of clinician, we selected with the following pri-
ing patients choice, disclosing clinician credentials, collecting ad- ority: dermatologist > primary care physician > other physi-
equate medical history, following evidence-based guidelines, co- cian > nurse practitioner > physician assistant. The initial HPI
ordinating care with existing treating physicians, and establish- was submitted in its entirety if there was any opportunity to
ing protocols for local referrals.13-16 We assessed the performance enter it, and was supplemented with the additional history if
of DTC telemedicine websites and apps by submitting a series of opportunities were given to enter an ROS or if relevant addi-
structured dermatologic consultations. tional questions were asked. At least 1 of the photographs was
submitted if there was any way to do so, and additional pho-
tographs were also uploaded if the website specified that 2 or
3 photographs were preferable.
Methods We recorded data from each encounter related to fees paid,
We performed a series of internet searches seeking DTC telemedi- response times, choice of clinician, transparency of credentials,
cine websites and smartphone apps accepting patient-originated clinician location, demographic and medical data requested, di-
visits for skin conditions. For inclusion, websites had to offer ser- agnoses given, treatments prescribed, adverse effects discussed,
vices to California residents and mention skin disease among referrals made, and medical records made available. When pro-
treated conditions. Websites were excluded if they required live- vided with a clinician name and location but not credentials, we
interactive video, a specific enrolled employer, or communica- used searches of state licensure databases, national board cer-
tion from a referring clinician. We also excluded websites with tification databases, and other websites to attempt to establish
just 1 clinician, only serving a clinic’s existing patients, or primar- licensure and board certification status. No prescriptions were
ily offering custom medication compounding. ever procured by study personnel.
Six simulated structured dermatologic cases were con- The institutional review board of the University of California,
structed, each including patient demographics, history of present San Francisco, reviewed and approved the study protocol.
illness (HPI), review of systems (ROS), and 3 photographs of skin
eruptions or lesions. The photographs were mostly obtained from
publicly available online image search engines, which any patient
wanting to obtain prescriptions from a DTC telemedicine web-
Results
site could access, copy, and submit. To simulate the information Sixteen DTC telemedicine websites and apps met inclusion cri-
that real patients present during both in-person and virtual inter- teria and responded to at least 1 case (Box 1). A few others met
E2 JAMA Dermatology Published online May 15, 2016 (Reprinted) jamadermatology.com
Copyright 2016 American Medical Association. All rights reserved.
Downloaded From: http://archderm.jamanetwork.com/ by a UCSF LIBRARY User on 05/15/2016
Direct-to-Consumer Telemedicine Websites Treating Skin Disease Original Investigation Research
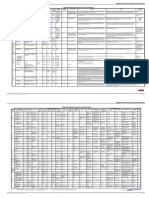
Table 1. Structured Clinical Case Descriptions of 6 Simulated Patients
Patient Age, y/Sex/Occupation Additional History Offered if Asked or Submitted
and Diagnosis Initial HPI Given if Opportunity to Enter in ROS
28/F/Freelance writer with acne in I’ve had acne since my teen years but now I’m 28 and Irregular periods ranging from 4 to 10 weeks apart,
setting of undiagnosed PCOS I’m getting tired of it. I tried a bunch of prescription sometimes skips a month.
creams and ointments (like clindamycin and Retin-A) I have more hair growth on my face than my friends; I get
that didn’t work, and an antibiotic pill (I’m not sure electrolysis on my chin and jawline.
which kind) I took for a few months a couple of years I use condoms, no current or prior OCPs, no prior pregnancies.
ago made it halfway better. What can I do to get clearer My mom has diabetes.
skin?
25/M/Waiter with annular secondary I have a bad new rash. I saw my regular doctor and she No prior similar rashes.
syphilis plaques said it is psoriasis, but the cream she gave me (desonide) Mostly protected sex with 1 male partner, but occasional
isn’t helping much. It all started about 3 weeks ago unprotected sex with others.
when it broke out on my back, chest, arms, legs, and No oral lesions.
feet. It doesn’t really itch that much, but I look terrible. I get herpes sores on my penis every few months, last was 2
It’s even all in my scalp, and the desonide cream just months ago, none now.
makes a mess of my hair. A couple of weeks ago, I had a headache and felt feverish for
a couple of days, but it is better now.
Last HIV test 6 months ago, negative result.
No arthralgias, no nail changes.
Current medications: Desonide cream.
20/M/College student with I’ve had acne since I was 12. Two years ago, my Right before this breakout, I ran out of doxycycline for 2
gram-negative folliculitis due to acne dermatologist started me on pills (doxycycline) and it weeks, but I restarted the pills 6 weeks ago, and they aren’t
antibiotics was awesome. It was so much better for a long time. I’m helping anymore.
still on the pills, but my acne has been getting bad again No truncal acne.
on my lips and chin with some new pus bumps for 2 No other symptoms.
months. Why isn’t it working anymore? What else can I No medication adverse effects except sunburn from the
use? doxycycline last year.
No new topicals or cosmetics being put on face.
Similar to prior acne? No, this breakout is totally different.
35/M/Barista with both a nodular There are 2 moles that I wanted you to check. Do I need Growth? Not sure, maybe they are 25% bigger
melanoma and a seborrheic keratosis to get them taken off? One is on my right cheek, the Change? I’m not sure, wasn’t really looking at them much
other is in the middle of my back. I think they both before. One seems round, the other kind of oval. Painful? No.
showed up about 5 years ago, but I’m not sure. They Itchy? No. Bleeding? No.
both seem to have grown some this year, but they don’t Lots of other moles? I have 20 or so total.
hurt or itch or anything. Previous skin biopsies? No, I’ve never seen a dermatologist.
Anybody in the family with skin cancer? No
Sun exposure history? I guess I got a few sunburns when I
was a teenager on vacation, I’m not sure how many.
Indoor tanning history? Nope, I never did that.
Current medications? Cymbalta.
19/F/Student and waiter with eczema I’ve had eczema since I was a little kid. It’s been pretty Blisters? Maybe, my skin is oozing a lot.
herpeticum bad at times. But it was getting better over the last year History of cold sores? I don’t think so.
or 2. My creams had been working pretty well. Over the History of genital lesions? No
past 10 days, my skin on my face and neck got way more Fever or other symptoms: I felt a little warm lately, but
itchy and irritated and my rash got worse. Do I need a haven’t taken my temperature, and don’t have a thermometer
stronger cream? Should I start on Atarax pills again? around. No other symptoms.
Do the new bumps hurt? They do sting .
Eye lesions or soreness? No.
Has your eczema been on your face or neck in the past? I’ve
had it just about everywhere.
Ever had any immune system problems? No.
Positive personal history of asthma. My mom and sister both
had eczema.
Current medications? Desonide face, triamcinolone
extremities.
60/M/Retired high school coach with These red splotches on my legs have been there a couple Does it itch? Yeah, at night.
stasis dermatitis of months, and this week they turned brighter red and Is it warm/hot? Seems like it. Yeah, it does feel a little warm.
got all irritated. My wife thinks it has started to get How fast is it spreading? I don’t know, it took a few days to
bigger. Is this an infection? Do I need antibiotics? get bigger.
Fever, sweats, chills? No.
Any other rashes? No.
Any surgical procedures? None other than my appendix
removal.
Leg swelling? I always have a little bit, but this is making it
worse.
Any medicine tried? I tried some Gold Bond cream for the last
3 days, but I don’t know if it did anything.
Current medications? Diovan, hydrochlorothiazide, Zocor.
Abbreviations: HIV, human immunodeficiency virus; HPI, history of present illness; OCP, oral contraceptive pill; PCOS, polycystic ovarian syndrome;
ROS, review of systems.
inclusion criteria but failed to respond to requests or had por- submissions but not others), and inconsistent replies (some web-
tal error messages that prevented successful case submission sites only intermittently replied). No website asked for photo-
(Figure). graphic identification or raised any concerns that the patient had
There were 62 clinical cases with a successful submission and used a pseudonym or submitted false photographs.
response.Nonrespondersweretheresultofscopelimitations,pay- The price per consultation varied—most charged a fixed
ment problems (a few websites accepted gift debit cards on some cost per visit ($35-$95), while others charged monthly
jamadermatology.com (Reprinted) JAMA Dermatology Published online May 15, 2016 E3
Copyright 2016 American Medical Association. All rights reserved.
Downloaded From: http://archderm.jamanetwork.com/ by a UCSF LIBRARY User on 05/15/2016
Research Original Investigation Direct-to-Consumer Telemedicine Websites Treating Skin Disease
Figure. Sample, Excluded Websites, Nonresponders, and Responders
Box 1. Direct-to-Consumer Telemedicine Website
and App Respondents
30 Direct-to-consumer telemedicine
Dermatology only websites that offered telemedicine
services to California residents for
• DermatologistOnCall skin diseases
• Dermcheck (phone app only)
• DermLink 11 Excluded
• Direct Dermatology 3 Required live interactive video
• First Derm 1 Required specific enrolled employer
1 Required communication from
• SkyMD referring clinician
• Spruce (phone app only) 2 Only 1 clinician performed all consults
• Virtual Acne (acne only) 2 Only served brick-and-mortar clinic’s
existing patients
• YoDerm (acne only) 2 Primarily offered custom medication
compounding
General medical websites
• Amwell
• First Opinion (phone app only) 19 Telemedicine websites to which cases
were submitted
• HealthTap Prime
• MD Live
3 Did not respond
• MeMD 1 Failed to respond to any request
• Teladoc 2 Portal error messages prevented
• Virtuwell all submissions
16 Telemedicine websites responded
to ≥1 case submission
memberships ($9 per 2 weeks to $49 monthly). Response times
were rapid (0-8 days), with 87% of encounters receiving re-
plies on the same or following day. 88 Consultations requested
14 Websites were each sent 6 cases
Websites allowed patients to select a clinician on 20 of 62 2 Acne cases
encounters (32%), while the remaining 42 (68%) assigned a cli- 4 Non-acne cases
2 Websites were each sent 2 acne
nician without any patient choice. We were able to determine cases only
the practice type of the clinician in all but 5 encounters (57 of
62 encounters). Physician backgrounds included dermatol- 14 Consultations excluded (unable to submit
due to credit card payment failure)
ogy (27), internal medicine (5), emergency medicine (3), fam-
ily medicine (3), obstetrics/gynecology (1), cardiology (1), pain 74 Consultations successfully submitted
management (1), and physical medicine/rehabilitation (1). The
nonphysician backgrounds included family nurse practition- 12 Consultations excluded
ers (3), physician assistants from dermatology settings (3), and 8 No response
4 Cases declined by clinicians
a nurse practitioner in emergency medicine. The rest were 2 Cases considered out of scope
primary care physicians in India (6) and dermatologists in 1 Required >3 photographs
1 Only treated existing patients
Sweden (2).
For the 49 identified US-based clinicians, we were able to 62 Consultations included in the analysis
confirm that all were licensed in California. Only 16 of the en-
counters (26%) disclosed information about licensure. Board
certification was disclosed for 20 of the 42 known domestic
MD encounters, and we were able to subsequently verify patient relationship,” but we found that they did make diag-
American Board of Medical Specialties (ABMS) board certifi- noses and offer specific treatment recommendations (without
cation in the declared specialty for 39 of these. sending prescriptions to pharmacies).
The clinician’s geographic practice location was disclosed The demographic and clinical data collected by the web-
in 38 encounters (61%). We were able to determine the loca- sites are summarized in Table 2. In very few of the encoun-
tion for 57 encounters, 35 of which were in California (11 within ters did the clinician ask the name of an existing primary care
100 miles of the patient). The remaining locations included In- physician (23%) or dermatologist (2%), and only 6 of 62 (10%)
dia (6), Minnesota (4), Colorado (3), Illinois (2), Washington, DC ultimately offered to send records to a current member of the
(2), Vermont (2), Sweden (2), and New York (1). patient’s clinical team. While all encounters allowed the pa-
The 8 internationally based physicians who were not Cali- tient to give some history, only 21 sought any ROS (34%). Forty-
fornia-licensed and provided responses worked for First Opin- six (74%) collected medication or allergy lists, and only 11 (52%)
ion or First Derm, both of which are headquartered in Califor- asked female patients about pregnancy or lactation status. Most
nia. First Derm claims their physicians are “board-certified encounters allowed our patients to submit photographs, re-
dermatologists,” but we were unable to find evidence that they questing 1 to 3 images. Clinicians in 4 encounters, however,
were either licensed in California or were ABMS certified. These provided diagnoses based solely on a submitted medical his-
websites post a variety of disclaimers that they do “not pro- tory without asking for or offering the chance to upload any
vide health care services,” and do “not create a physician- images. These diagnoses without images were provided by a
E4 JAMA Dermatology Published online May 15, 2016 (Reprinted) jamadermatology.com
Copyright 2016 American Medical Association. All rights reserved.
Downloaded From: http://archderm.jamanetwork.com/ by a UCSF LIBRARY User on 05/15/2016
Direct-to-Consumer Telemedicine Websites Treating Skin Disease Original Investigation Research
menses by a single website (1 website inquired about menses
Table 2. Percentage of Encounters Requiring Specific Demographic
or Clinical Information only to check pregnancy status before prescribing). Every
clinician diagnosed acne, including 1 who did not ask for
Type of Data Collected No. (%)
photographs, and none raised the issue of hirsutism, andro-
Demographic data
gen excess, or PCOS. Two of 12 websites responding to this
Patient name 57 (92)
case recommended in-person follow-up for treatment, and 1
Street address 33 (53)
recommended use of only mild soaps, moisturizers, and cool
City/state 56 (90)
showers. The patient received prescriptions for oral antibiot-
Phone No. 44 (71) ics (from 8 websites), topical retinoids (6), and topical antibi-
Age or date of birth 62 (100) otics (5). None of the clinicians discussed hormonal treat-
Social security No. 0 ment options.
Driver’s license No. 0 In the case of secondary syphilis with unusual plaques, the
Occupation 6 (10) patient was not asked about his recent fever (even when he pro-
Name of existing PCP 14 (23) actively reported it on ROS), and no clinician seemed con-
Address of existing PCP 3 (5) cerned that his diffuse eruption began so acutely only 3 weeks
Fax of existing PCP 7 (11) previously without a history of prior skin eruptions (uncom-
Name of existing dermatologist 1 (2) mon in patients with large-plaque psoriasis). Seven of the 8 cli-
Address of existing dermatologist 1 (2) nicians diagnosed psoriasis, including 1 who did not ask for
Fax No. of existing dermatologist 1 (2) photographs. One clinician (an emergency physician) made no
Local pharmacy 48 (77) diagnosis and referred the patient to see a local dermatolo-
Insurance status 25 (40) gist, and another (a Sweden-based physician) who diagnosed
Clinical data psoriasis suggested that the patient see a local dermatologist
History of present illness 62 (100)
for treatment. This patient received prescriptions for class I or
II topical steroids in 5 encounters and was told to use mois-
Review of systems 21 (34)
turizers and take lukewarm baths in another.
Medical history 41 (66)
In the case of gram-negative folliculitis, 1 clinician (a board-
Surgical history 12 (19)
certified dermatologist) referred the patient to a local derma-
Skin cancer history 7 (11)
tologist for a culture, and another (an India-based physician)
Family history 20 (32)
sent him to his primary care physician for diagnosis. The re-
Current medication list 46 (74)
maining 10 clinicians all diagnosed acne, seemingly uncon-
Allergies 46 (74)
cerned by the sudden appearance of pustules around the
Pregnancy statusa 11 (52)a
mouth after lengthy doxycycline use (a common presenta-
a
Lactation status 11 (52)a tion of gram-negative folliculitis caused by Proteus, Klebsiella,
Abbreviation: PCP, primary care physician. or Serratia). This patient was prescribed trimethoprim-
a
Denominator includes only the 21 encounters with a female patient. sulfamethoxazole (by 2 clinicians), minocycline (by 3), con-
tinued doxycycline (by 1), topical antibiotics (by 3), and topi-
board-certified physical medicine/rehabilitation physician (1), cal retinoids (by 2). One clinician suggested only topical retinol,
board-certified internist (1), and physicians located in India (2). and another recommended reducing his sugar intake and ap-
A diagnosis or likely diagnosis was proffered in 48 (77%) of plying moisturizer.
encounters, with the remainder of patients being referred to a In the patient with 1 nodular melanoma and 1 seborrheic
local physician for diagnosis. Patients referred for diagnosis were keratosis, 11 of 14 clinicians referred the patient for an in-
given suggested name(s) of practicing local clinicians in only 2 person examination of at least 1 of his lesions. The others
of 14 instances. No patients were sent to a laboratory for stud- (2 dermatologists and a physician assistant) reassured him that
ies. A differential diagnosis was listed in 8 of 48 cases with di- both lesions were benign.
agnoses (17%), and 2 of 14 cases without diagnoses (14%). The young woman with eczema herpeticum blisters (a po-
Among 48 encounters with diagnoses, 31 (65%) were given tentially life-threatening infection caused by herpes simplex
prescription medications, and 9 (19%) were told to seek a lo- virus erupting in eczema) was diagnosed as having an ordi-
cal physician for treatment (3 gave suggested names). The re- nary eczema flare or contact allergies in 7 of 9 encounters, but
mainder were reassured, treated with over-the-counter medi- 2 clinicians (1 dermatologist, 1 unidentified) raised concerns
cations, or had prescriptions recommended but not provided. about infection and referred her to be seen in person (though
When prescriptions were provided, the clinician disclosed rel- they did not suggest any timeline or individuals she could see).
evant adverse effects or risks in 10 of 31 encounters (32%). She was prescribed oral prednisone (2), topical steroids (2), and
Among 14 encounters where a female patient was prescribed antihistamines (1). Of the remaining 2 websites that diag-
a pregnancy class C or higher drug, pregnancy risks were dis- nosed eczema, one recommended that topical steroids be pre-
closed in 6 (43%). scribed in person, and the other recommended a vegan diet
In the case of polycystic ovarian syndrome (PCOS) with and suggested follow-up with an allergist. The 2 clinicians rec-
inflammatory acne, the 28-year-old patient was not asked ommending prednisone, which can worsen eczema herpeti-
relevant questions about her hypertrichosis or irregular cum when given without antiviral drugs, and which clinical
jamadermatology.com (Reprinted) JAMA Dermatology Published online May 15, 2016 E5
Copyright 2016 American Medical Association. All rights reserved.
Downloaded From: http://archderm.jamanetwork.com/ by a UCSF LIBRARY User on 05/15/2016
Research Original Investigation Direct-to-Consumer Telemedicine Websites Treating Skin Disease
guidelines recommend avoiding even for uninfected atopic der- suggested where patients might go in a small minority of cases.
matitis, were a doctor of osteopathic internal medicine and a None offered to actually facilitate a referral to a local physi-
family nurse practitioner. cian (except in 1 instance where the clinician self-referred), even
The patient with stasis dermatitis was properly diag- when some of the clinical scenarios involved urgent medical
nosed by all 7 websites where his case was successfully sub- conditions in which ensuring follow-up was vital. This lack of
mitted. He was prescribed topical clobetasol (3) or hydrocor- care coordination may be related to the substantial geo-
tisone (2). One website suggested clobetasol but did not provide graphic distance of many of the clinicians from our simulated
a prescription, and 1 website suggested he see a local physi- patients and their possible lack of knowledge of the local health
cian for a cardiac workup. care system.
Many patients were prescribed oral or topical medica-
tions, and only one-third were told about relevant risks or ad-
verse effects. Fewer than half of pregnancy category C or higher
Discussion prescriptions given to women of childbearing age included any
When implemented appropriately, DTC telemedicine web- discussion of pregnancy risks or avoidance.
sites can improve access to quality care for patients facing geo- One dominant pattern emerged when examining the di-
graphic, mobility, or financial constraints. While a large body agnostic accuracy of these websites with our clinical sce-
of evidence supports the use of teleconsultation for skin dis- narios. For the 2 cases in which photographs alone were ad-
ease between a referring clinician and dermatologist, our study equate to easily make a correct diagnosis (stasis dermatitis and
raises significant concerns about the rapidly expanding use of melanoma), most of the DTC telemedicine websites per-
direct-to-consumer telemedicine. formed well. However, when further engaging the patient for
The DTC telemedicine websites we consulted, many with basic history elements was a necessary part of the interac-
a large and growing national footprint, provided care that of- tion, diagnostic performance was poor.
ten lacked patient choice of clinician, transparency of clini- None of the clinicians asked the 28-year-old woman with
cian credentials, or care coordination with existing health care inflammatory acne about her irregular menses or hirsutism,
teams. Many diagnoses were proffered without reasonable at- so none raised concerns about PCOS or androgen excess or ini-
tempts to ask basic medical history follow-up questions, treat- tiated appropriate treatment. The young man with highly in-
ment recommendations sometimes contradicted evidence- fectious secondary syphilis was not asked about his recent fe-
based guidelines, and prescriptions frequently lacked basic vers, attention was not paid to the unusually sudden onset he
disclosure of adverse effects, risks, or pregnancy warnings. described, and all but 1 of the websites accepted the diagno-
When referrals to in-person care were made, they rarely in- sis of psoriasis the patient himself offered. This not only left
cluded suggested clinician names. No DTC telemedicine web- him at substantial risk from untreated syphilis, but was a pub-
sites attempted to confirm the identity of patients or raised lic health failure given the urgent need for contact tracing and
doubts about the authenticity of photographs. risks of ongoing transmission. The patient with gram-
Patient choice of their treating physician is part of our medi- negative folliculitis was not given a chance to say that the ram-
cal code of ethics,17 and we were surprised that these web- pant new pustules around his mouth were unlike the acne he
sites with multiple clinicians on staff assigned a clinician with- had before. The patient with eczema herpeticum faces the risk
out patient choice in most encounters. Transparency about of disseminated infection and even death (especially when
licensing and credentials is inherent in patient choice and in- given systemic steroids without antiviral drugs) because most
formed consent, and most services failed to provide licen- of the DTC telemedicine clinicians did not ask about the sting-
sure or board certification information during encounters. De- ing vesicles shown in her photographs.
spite claims that they were not providing health care services, Our study has a significant limitation: we are unable to
we believe that 2 DTC telemedicine websites headquartered assess whether clinicians seeing these patients in traditional
in California but using foreign clinicians were engaged in the in-person encounters would have performed better on diag-
practice of medicine without a state license, as they clearly pro- nostic accuracy. However, the additional medical history
vided diagnoses and treatment recommendations. necessary to make the diagnoses (eg, fevers, irregular men-
Our findings also suggest that treatment provided by these ses) are the types of information that, in our experience,
websites is likely to exacerbate care fragmentation, since only typically emerge in the give-and-take of obtaining a history
23% asked for the names of existing primary care physicians, in the office setting. This give-and-take could certainly be
and only 10% offered to provide medical records to existing replicated in a store-and-forward telemedicine environ-
clinicians. In an era when traditional health care delivery is ment, especially if the clinician takes time to engage the
working to “minimize silos” (ie, individuals, groups, organi- patient, but the DTC telemedicine websites we queried typi-
zations, or systems that operate in isolation, lacking ad- cally offered diagnoses and prescriptions immediately after 1
equate communication with other groups) and improve inad- form-driven submission, without sending meaningful,
equate care coordination, it makes little sense to design new appropriate follow-up questions to our simulated patients.
care delivery channels without including an ability for pa- In addition, diagnostic inaccuracy is only 1 of many concern-
tients’ longitudinal care teams to know about new diagnoses ing outcomes we reported.
made and treatments initiated. When DTC telemedicine web- Another limitation of our study is that the design forced
sites determined that in-person care was necessary, they only us to exclude any DTC telemedicine websites or apps that re-
E6 JAMA Dermatology Published online May 15, 2016 (Reprinted) jamadermatology.com
Copyright 2016 American Medical Association. All rights reserved.
Downloaded From: http://archderm.jamanetwork.com/ by a UCSF LIBRARY User on 05/15/2016
Direct-to-Consumer Telemedicine Websites Treating Skin Disease Original Investigation Research
quired live interactive video. However, only 3 DTC telemedi-
cine websites from our initial search had to be excluded for re- Box 2. Authors’ Recommended Practices for Direct-to-Consumer
quiring video. We also excluded platforms serving only a clinic’s Telemedicine Websites
existing patients, which may be expected to offer more coor- • Disclose the licensure, credentials, and location of their clinicians,
dinated care. making sure that all are licensed in the states where patients are
Finally, we cannot fully guarantee the photographs ac- located, and give patients some choice of which clinician will
quired from the internet are of patients with biopsy or labo- provide their care.
ratory proof of the listed diseases. However, the fact that most • Obtain proof of identity of patients seeking care, and establish an
initial relationship with live interactive video before beginning a
DTC telemedicine websites failed to consider a diagnosis of ec-
store-and-forward relationship (when a patient’s existing health
zema herpeticum in a young woman with eczema and new ooz- care team is uninvolved).
ing, stinging blisters seems far more important than whether • Collect relevant medical history, including at least a history of
we have evidence of a positive Herpes culture from this woman present illness, review of systems, medication list, and drug
with a classic presentation in her photographs. allergies. In many instances, appropriate past medical records
should be available to the consulting clinician.
• Recognize that the accurate diagnosis of disease often requires
an interactive history, and train participating clinicians to ask
Conclusions appropriate follow-up questions to complete a patient’s relevant
medical history.
Telemedicine has potential to expand access, and the medi- • Seek the use of laboratory studies in clinical scenarios when an
cal literature is filled with examples of telehealth systems pro- in-person physician would have relied on those studies.
viding quality care. Our findings, however, raise doubts about • Provide diagnoses and treatments consistent with existing
the quality of skin disease diagnosis and treatment being pro- evidence-based guidelines.
• Engage in meaningful informed consent, including discussion of
vided by a variety of DTC telemedicine websites and apps. The
risks, potential adverse effects, pregnancy concerns, and a clear
substantial investment of health plans in providing enrollees
follow-up plan when prescribing medications.
with insurance-covered access to these DTC telemedicine web- • Collect information about a patient’s existing health care team
sites, as well as rapidly expanding availability for patients will- and provide medical records to relevant team members—unless a
ing to pay out of pocket over the internet, may be premature. patient opts out.
The problem may be exacerbated by several health plans’ will- • Have relationships with local physicians in all areas where they
ingness to pay large national DTC telemedicine providers while treat patients, so that patients are not sent to emergency
departments or left on their own when they need
excluding asynchronous telemedicine provided by a pa-
urgent in-person follow-up or experience medication adverse
tient’s existing specialists. effects.
We believe that DTC telemedicine can be used effec- • Create quality assurance programs that regularly monitor clinical
tively, but it is best performed by physicians and team performance, patient outcomes, follow-up, and care
members who are part of practices or regional systems in coordination.
which patients already receive care. This allows telemedi-
cine clinicians to view a patient’s existing medical records,
communicate with existing health care team members, pro- companies and participating clinicians improve their services so
vide in-person follow-up when needed, and be accountable that patients seeking these newer channels of care delivery can
for the care they deliver. A regional clinician network can receive transparent, ethically provided, coordinated, high-quality
provide a safety net for patients when errors in diagnosis care. In the meantime, we also hope that policymakers, regula-
and treatment occur. tors, and payers will find ways to identify and encourage tele-
Based on our findings, we believe that DTC telemedicine ser- medicine services that abide by these principles, while discour-
vices should, at a minimum, adopt several standard practices (Box aging the growth of DTC telemedicine websites and apps that
2). We hope that studies such as ours will help DTC telemedicine provide fragmented, low-quality care.
ARTICLE INFORMATION Administrative, technical, or material support: Role of the Funder/Sponsor: The American
Accepted for Publication: April 23, 2016. Abrouk, Lee. Academy of Dermatology Association had no role in
Study supervision: Abrouk, Lee, Kovarik. the design and conduct of the study; collection,
Published Online: May 15, 2016. management, analysis, and interpretation of the
doi:10.1001/jamadermatol.2016.1774. Conflict of Interest Disclosures: Dr Resneck serves
on the Board of Trustees of the American Medical data; preparation, review, or approval of the
Author Contributions: Dr Resneck had full access Association. Drs Resneck, Lee, Kovarik, and Edison manuscript; and decision to submit the manuscript
to all the data in the study and takes responsibility serve on the Telemedicine Task Force of the for publication.
for the integrity of the data and the accuracy of the American Academy of Dermatology Association. Dr Disclaimer: The views expressed in this article are
data analysis. Lee serves as a physician performing consultations those of the authors and do not necessarily
Study concept and design: Resneck, Abrouk, Lee, for Direct Dermatology but did not participate in represent the views of the American Medical
Kovarik, Edison. any of the telemedicine consultations Association or the American Academy of
Acquisition, analysis, or interpretation of data: encompassed in this study. No other disclosures are Dermatology Association (Dr Resneck is a trustee of
Resneck, Abrouk, Steuer, Tam, Yen. reported. the American Medical Association).
Drafting of the manuscript: Resneck, Abrouk.
Critical revision of the manuscript for important Funding/Support: The American Academy of
intellectual content: All authors. Dermatology Association provided funding for the
Obtained funding: Resneck. debit cards used in the study.
jamadermatology.com (Reprinted) JAMA Dermatology Published online May 15, 2016 E7
Copyright 2016 American Medical Association. All rights reserved.
Downloaded From: http://archderm.jamanetwork.com/ by a UCSF LIBRARY User on 05/15/2016
Research Original Investigation Direct-to-Consumer Telemedicine Websites Treating Skin Disease
REFERENCES 7. Digital Health Funding 2015 Year in Review. Rock 13. American Medical Association. H-480.946
1. Warshaw EM, Gravely AA, Nelson DB. Reliability Health. http://rockhealth.com/reports/digital Coverage of and payment for telemedicine. https:
of store and forward teledermatology for skin -health-funding-2015-year-in-review/. Accessed //www.ama-assn.org/ssl3/ecomm
neoplasms. J Am Acad Dermatol. 2015;72(3):426-435. March 31, 2016. /PolicyFinderForm.pl?site=www.ama-assn.org&uri
8. Dolan B. InDepth: The Changing Relationship of =/resources/html/PolicyFinder/policyfiles/HnE/H
2. Edison KE, Ward DS, Dyer JA, Lane W, Chance L, -480.946.HTM. Accessed March 31, 2016.
Hicks LL. Diagnosis, diagnostic confidence, and Health Plans and Virtual Visit Services. MobiHealth
management concordance in live-interactive and News. September 11, 2015. http://mobihealthnews 14. American Academy of Dermatology
store-and-forward teledermatology compared to .com/46676/in-depth-the-changing-relationship Association. Position statement on
in-person examination. Telemed J E Health. 2008; -of-health-plans-and-virtual-visit-services. teledermatology (amended March 7, 2016). https:
14(9):889-895. Accessed March 31, 2016. //www.aad.org/Forms/Policies/Uploads/PS/PS
9. Huff C. AARP Bulletin. Medical Diagnosis by -Teledermatology.pdf. Accessed March 31, 2016.
3. Warshaw EM, Gravely AA, Bohjanen KA, et al.
Interobserver accuracy of store and forward Webcam? Telemedicine exams are fast and 15. Daniel H, Sulmasy LS; Health and Public Policy
teledermatology for skin neoplasms. J Am Acad easy—but questions remain. December 2015. http: Committee of the American College of Physicians.
Dermatol. 2010;62(3):513-516. //www.aarp.org/health/conditions-treatments Policy recommendations to guide the use of
/info-2015/telemedicine-health-symptoms telemedicine in primary care settings: an American
4. Datta SK, Warshaw EM, Edison KE, et al. Cost -diagnosis.html. Accessed March 31, 2016. College of Physicians position paper. Ann Intern Med.
and utility analysis of a store-and-forward 2015;163(10):787-789.
teledermatology referral system: a randomized 10. Uscher-Pines L, Mulcahy A, Cowling D,
clinical trial. JAMA Dermatol. 2015;151(12):1323-1329. Hunter G, Burns R, Mehrotra A. Access and quality 16. Marcin JP, Rimsza ME, Moskowitz WB;
of care in direct-to-consumer telemedicine. Committee on Pediatric Workforce. The use of
5. Whited JD, Warshaw EM, Kapur K, et al. Clinical Telemed J E Health. 2016;22(4):282-287. telemedicine to address access and physician
course outcomes for store and forward workforce shortages. Pediatrics. 2015;136(1):
teledermatology versus conventional consultation: 11. Kochmann M, Locatis C. Direct to consumer
mobile teledermatology apps: an exploratory study 202-209.
a randomized trial. J Telemed Telecare. 2013;19(4):
197-204. [published online March 9, 2016]. Telemed J E Health. 17. American Medical Association. Code of Medical
doi:10.1089/tmj.2015.0189. Ethics. Opinion 9.06—Free Choice. http://www
6. Pak H, Triplett CA, Lindquist JH, Grambow SC, .ama-assn.org/ama/pub/physician-resources
Whited JD. Store-and-forward teledermatology 12. Fogel AL, Sarin KY. A survey of
direct-to-consumer teledermatology services /medical-ethics/code-medical-ethics/opinion906
results in similar clinical outcomes to conventional .page. Accessed April 3, 2016.
clinic-based care. J Telemed Telecare. 2007;13(1): available to US patients: explosive growth,
26-30. opportunities and controversy [published online
January 4, 2016]. J Telemed Telecare.
doi:10.1177/1357633X15624044.
E8 JAMA Dermatology Published online May 15, 2016 (Reprinted) jamadermatology.com
Copyright 2016 American Medical Association. All rights reserved.
Downloaded From: http://archderm.jamanetwork.com/ by a UCSF LIBRARY User on 05/15/2016
Das könnte Ihnen auch gefallen
- Lyme, Tick Borne Diseases & Mental Symptoms, AutismDokument81 SeitenLyme, Tick Borne Diseases & Mental Symptoms, AutismjinooNoch keine Bewertungen
- O RadsDokument15 SeitenO RadsMurilo Campos100% (1)
- Christopher H. Wise - Mobilization Notes - A Rehabilitation Specialist's Pocket GuideDokument240 SeitenChristopher H. Wise - Mobilization Notes - A Rehabilitation Specialist's Pocket GuideRukaphuongNoch keine Bewertungen
- Basic Nursing Fundamentals EliminationDokument35 SeitenBasic Nursing Fundamentals Eliminationlisa100% (1)
- OCDDokument51 SeitenOCDImon Paul100% (1)
- Pediatric DermatologyDokument568 SeitenPediatric DermatologyLuiza Radulescu89% (9)
- Psychological DisordersDokument21 SeitenPsychological DisordersMark100% (2)
- ACR Thyroid Imaging, Reporting and Data 2018 TesslerDokument9 SeitenACR Thyroid Imaging, Reporting and Data 2018 TesslerdianaveebaeNoch keine Bewertungen
- Efficacy of An Intervention To Alter Skin Cancer Risk Behaviors in Young AdultsDokument11 SeitenEfficacy of An Intervention To Alter Skin Cancer Risk Behaviors in Young AdultsChRinaldoNoch keine Bewertungen
- Classifi Cation of Treatment-Related Mortality in Children WithDokument7 SeitenClassifi Cation of Treatment-Related Mortality in Children WithIgnatia Rosalia KiranaNoch keine Bewertungen
- Lester 2010Dokument8 SeitenLester 2010Riska Resty WasitaNoch keine Bewertungen
- Early-Onset Basal Cell Carcinoma and Indoor Tanning: A Population-Based StudyDokument9 SeitenEarly-Onset Basal Cell Carcinoma and Indoor Tanning: A Population-Based StudyHinami TenukiNoch keine Bewertungen
- Sessionsetal High Alert Meds 919 JANDokument15 SeitenSessionsetal High Alert Meds 919 JANichabojanNoch keine Bewertungen
- HHS Public AccessDokument11 SeitenHHS Public AccessYTHNoch keine Bewertungen
- AMP CancerDokument20 SeitenAMP Cancerprateek bhatiaNoch keine Bewertungen
- AI in Cancer ImagingDokument31 SeitenAI in Cancer ImagingHeriberto AguirreNoch keine Bewertungen
- Trichomonas Vaginalis: Common, Curable and in The Diagnostic SpotlightDokument23 SeitenTrichomonas Vaginalis: Common, Curable and in The Diagnostic SpotlightMahmoud HakimNoch keine Bewertungen
- The Evolving Role of Primary Care Practitioners in DermatologyDokument5 SeitenThe Evolving Role of Primary Care Practitioners in DermatologyafbmgNoch keine Bewertungen
- Journal of Ajog PDFDokument13 SeitenJournal of Ajog PDFBima MahardhikaNoch keine Bewertungen
- Articulo 1 LinfedemaDokument7 SeitenArticulo 1 LinfedemaMateo GonzalezNoch keine Bewertungen
- Azad 2019Dokument7 SeitenAzad 2019Eka BagaskaraNoch keine Bewertungen
- Melanoma in Clinical PracticeVon EverandMelanoma in Clinical PracticeRhoda M. AlaniNoch keine Bewertungen
- Evaluation of Point-of-Care Decision Support For Adult Acne Treatment by Primary Care CliniciansDokument7 SeitenEvaluation of Point-of-Care Decision Support For Adult Acne Treatment by Primary Care CliniciansbellaNoch keine Bewertungen
- Cancer - 2003 - Mitby - Utilization of Special Education Services and Educational Attainment Among Long Term Survivors ofDokument12 SeitenCancer - 2003 - Mitby - Utilization of Special Education Services and Educational Attainment Among Long Term Survivors ofLayla FassarellaNoch keine Bewertungen
- Patient-Reported Dysphagia After Thyroidectomy A Qualitative StudyDokument7 SeitenPatient-Reported Dysphagia After Thyroidectomy A Qualitative StudybatviserNoch keine Bewertungen
- Screening For SyphilisDokument10 SeitenScreening For SyphilisAntonio Orquera AndradeNoch keine Bewertungen
- Early-Onset Basal Cell CarcinomaDokument11 SeitenEarly-Onset Basal Cell CarcinomajxmackNoch keine Bewertungen
- Communication Skill TrainingDokument6 SeitenCommunication Skill TrainingjjpulikenNoch keine Bewertungen
- PerioperativeDokument11 SeitenPerioperativeKarinaWijayantiNoch keine Bewertungen
- CA A Cancer J Clinicians - 2019 - BiDokument31 SeitenCA A Cancer J Clinicians - 2019 - BiMeeqatNoch keine Bewertungen
- The Role of Radiology in Diagnostic Error: A Medical Malpractice Claims ReviewDokument7 SeitenThe Role of Radiology in Diagnostic Error: A Medical Malpractice Claims ReviewEva HikmahNoch keine Bewertungen
- RosaceaVon EverandRosaceaJohn Havens CaryNoch keine Bewertungen
- Skin Cancer Prevention Education For Kidney Transplant Recipients: A Systematic Evaluation of Internet SitesDokument7 SeitenSkin Cancer Prevention Education For Kidney Transplant Recipients: A Systematic Evaluation of Internet SitesPrathita AmandaNoch keine Bewertungen
- Evidence 1 STDokument7 SeitenEvidence 1 STTania FigueroaNoch keine Bewertungen
- Patient Reported BarriesDokument14 SeitenPatient Reported Barriesdani catriaNoch keine Bewertungen
- Comment On “ The First 30  Years of TheDokument1 SeiteComment On “ The First 30  Years of TheYilianeth Mena DazaNoch keine Bewertungen
- Jurnal Mak Ta 1Dokument18 SeitenJurnal Mak Ta 1Ririn FebriantiNoch keine Bewertungen
- Research Paper of Skin CancerDokument8 SeitenResearch Paper of Skin Cancerruogdicnd100% (1)
- Hospitalizations For Ambulatory Care-Sensitive Conditions Among Children With Chronic and Complex DiseasesDokument7 SeitenHospitalizations For Ambulatory Care-Sensitive Conditions Among Children With Chronic and Complex DiseasesHasriana BudimanNoch keine Bewertungen
- A Systematic Review of Satisfaction With TeledermatologyDokument8 SeitenA Systematic Review of Satisfaction With Teledermatologysri karuniaNoch keine Bewertungen
- Oncology Nursing Trends and Issues 3Dokument7 SeitenOncology Nursing Trends and Issues 3DaichiNoch keine Bewertungen
- Jamadermatol 2018 5353Dokument6 SeitenJamadermatol 2018 5353barkahalamri52Noch keine Bewertungen
- 10 1016@j Mayocp 2018 03 002Dokument14 Seiten10 1016@j Mayocp 2018 03 002Jose AbadiaNoch keine Bewertungen
- Exploring Concerns of Children With CancerDokument7 SeitenExploring Concerns of Children With CancerVanessa SilvaNoch keine Bewertungen
- PrimaryCareProviderAwarenessofIR-A Single-Center AnalysisDokument8 SeitenPrimaryCareProviderAwarenessofIR-A Single-Center AnalysisQueen Arlene BeeNoch keine Bewertungen
- Evidence-Based Recommendations For The Diagnosis and Treatment of Pediatric AcneDokument26 SeitenEvidence-Based Recommendations For The Diagnosis and Treatment of Pediatric AcnezuliaahmadNoch keine Bewertungen
- Narrative Communication in Cancer Prevention and Control PDFDokument15 SeitenNarrative Communication in Cancer Prevention and Control PDFMuhammad SharjeelNoch keine Bewertungen
- Scms 6s 6-16 Hawaiisppl v9Dokument28 SeitenScms 6s 6-16 Hawaiisppl v9Michele CarvalhoNoch keine Bewertungen
- Availability of Essential Diagnostics in Ten Low-Income and Middle-Income CountriesDokument8 SeitenAvailability of Essential Diagnostics in Ten Low-Income and Middle-Income CountriesnavinkkaranNoch keine Bewertungen
- NCCN: Continuing Education: Accreditation StatementsDokument11 SeitenNCCN: Continuing Education: Accreditation StatementsHieu NguyenNoch keine Bewertungen
- Knowledge, Attitudes, and Practices of Bedside Nursing Staff PDFDokument4 SeitenKnowledge, Attitudes, and Practices of Bedside Nursing Staff PDFwindysandy100% (1)
- Preeclampsia Screening Evidence Report and Systematic Review For The US Preventive Services Task ForceDokument16 SeitenPreeclampsia Screening Evidence Report and Systematic Review For The US Preventive Services Task ForceRoberto López MataNoch keine Bewertungen
- Ascha - ASJ19 - Nonsurgical Management of Facial Masculinization and FeminizationDokument15 SeitenAscha - ASJ19 - Nonsurgical Management of Facial Masculinization and Feminizationallen.515Noch keine Bewertungen
- Chimerism: A Clinical GuideVon EverandChimerism: A Clinical GuideNicole L. DraperNoch keine Bewertungen
- Jamadermatology Li 2020 Oi 200007Dokument7 SeitenJamadermatology Li 2020 Oi 200007Francisco José Martínez OrtegaNoch keine Bewertungen
- Academic Emergency Medicine - 2020 - Ebell - Accuracy of Signs and Symptoms For The Diagnosis of Community AcquiredDokument14 SeitenAcademic Emergency Medicine - 2020 - Ebell - Accuracy of Signs and Symptoms For The Diagnosis of Community AcquiredOnilis RiveraNoch keine Bewertungen
- A Multilevel Primare CareDokument11 SeitenA Multilevel Primare CareJaime BusquetNoch keine Bewertungen
- CME Part IDokument15 SeitenCME Part IEkkapap UnityNoch keine Bewertungen
- Asccp Colposcopy Standards Colposcopy Quality.6Dokument7 SeitenAsccp Colposcopy Standards Colposcopy Quality.6milenaquevedolaNoch keine Bewertungen
- Hudson 2003Dokument10 SeitenHudson 2003Borja Recuenco CayuelaNoch keine Bewertungen
- Karla, Articulo 2-2Dokument13 SeitenKarla, Articulo 2-2Richard Alejandro OrellanaNoch keine Bewertungen
- Association of Digital Media Use With Subsequent SymptomsDokument9 SeitenAssociation of Digital Media Use With Subsequent SymptomsSonyaKaminskayaNoch keine Bewertungen
- Fertility Preservation in Pediatric Leukemia and LymphomaDokument11 SeitenFertility Preservation in Pediatric Leukemia and LymphomaElianaNoch keine Bewertungen
- 1 s2.0 S0885392418300411 MainDokument7 Seiten1 s2.0 S0885392418300411 Maincheatingw995Noch keine Bewertungen
- Acad Emerg Med 2019 26 7 719-31Dokument14 SeitenAcad Emerg Med 2019 26 7 719-31Fernando SousaNoch keine Bewertungen
- CADDRA ADHD Information Resources HandoutDokument2 SeitenCADDRA ADHD Information Resources HandoutMustafa AlmasoudiNoch keine Bewertungen
- Agent CharacteristicsDokument2 SeitenAgent Characteristicsyiaili1234100% (1)
- Biology LabDokument5 SeitenBiology LabRuth-AnnLambertNoch keine Bewertungen
- Delos Reyes - Grade 12 - EAPPDokument2 SeitenDelos Reyes - Grade 12 - EAPPzavriaNoch keine Bewertungen
- Antiemetics: Dr. Bikram TewariDokument31 SeitenAntiemetics: Dr. Bikram TewariRajkamal SarmaNoch keine Bewertungen
- Chapter 006Dokument5 SeitenChapter 006api-281340024Noch keine Bewertungen
- Betaine HCLDokument4 SeitenBetaine HCLPhilmalin2011Noch keine Bewertungen
- Typhoid Fever: Also Known As Enteric FeverDokument3 SeitenTyphoid Fever: Also Known As Enteric Feverchristian quiaoitNoch keine Bewertungen
- Daftar PustakaDokument2 SeitenDaftar PustakaDasep PadilahNoch keine Bewertungen
- Experimental Pharmacology: Irrational Drug CombinationsDokument5 SeitenExperimental Pharmacology: Irrational Drug CombinationsPrabangkara BillyNoch keine Bewertungen
- Principles of Risk Management and Insurance 12Th Edition Rejda Test Bank Full Chapter PDFDokument34 SeitenPrinciples of Risk Management and Insurance 12Th Edition Rejda Test Bank Full Chapter PDFJasonMoralesykcx100% (9)
- Signs of PregnancyDokument3 SeitenSigns of Pregnancysaivishwa20Noch keine Bewertungen
- Morning ReportDokument14 SeitenMorning ReportAyu KristinaNoch keine Bewertungen
- Practical Pain ManagementDokument13 SeitenPractical Pain ManagementfrancistsyNoch keine Bewertungen
- Abnormal Ob HandoutsDokument3 SeitenAbnormal Ob HandoutsBoy MadNoch keine Bewertungen
- Vitamin A DeficiencyDokument5 SeitenVitamin A DeficiencyElvisNoch keine Bewertungen
- Subgroup 3Dokument12 SeitenSubgroup 3John Mervin OliverosNoch keine Bewertungen
- New Microsoft Word DocumentDokument19 SeitenNew Microsoft Word DocumentAisha FakhryNoch keine Bewertungen
- Glomerular Diseases: DR Rashmi NazarethDokument49 SeitenGlomerular Diseases: DR Rashmi NazarethRohit RajeevanNoch keine Bewertungen
- ClonidineDokument4 SeitenClonidineJoshua GonzalesNoch keine Bewertungen
- Outcomes of COPDDokument6 SeitenOutcomes of COPDRISKINoch keine Bewertungen
- Body Dysmorphic Disorder: SymptomsDokument7 SeitenBody Dysmorphic Disorder: SymptomsamiraNoch keine Bewertungen
- Care Plan - Chronic PainDokument4 SeitenCare Plan - Chronic Painapi-246639896Noch keine Bewertungen
- Endocrine Part 2 DRAFTDokument6 SeitenEndocrine Part 2 DRAFTPreeti Joan BuxaniNoch keine Bewertungen
- Sas 21-30 HaDokument10 SeitenSas 21-30 HaRiam Carl AgunosNoch keine Bewertungen