Das könnte Ihnen auch gefallen
- COMPREHENSIVE NURSING ACHIEVEMENT TEST (RN): Passbooks Study GuideVon EverandCOMPREHENSIVE NURSING ACHIEVEMENT TEST (RN): Passbooks Study GuideNoch keine Bewertungen
- Points in Community Health NursingDokument9 SeitenPoints in Community Health NursingkuyarahimNoch keine Bewertungen
- Leaping the Hurdles: The Essential Companion Guide for International Medical Graduates on their Australian JourneyVon EverandLeaping the Hurdles: The Essential Companion Guide for International Medical Graduates on their Australian JourneyNoch keine Bewertungen
- Fetal Alcohol Syndrome Brochure For Nursing SchoolDokument2 SeitenFetal Alcohol Syndrome Brochure For Nursing SchoolKrystal Cowley Miller100% (1)
- CHNDokument38 SeitenCHNLouie John AbilaNoch keine Bewertungen
- CHN, Gapuz BookDokument10 SeitenCHN, Gapuz BookNia KayeNoch keine Bewertungen
- PN FUNDAMENTALS: Passbooks Study GuideVon EverandPN FUNDAMENTALS: Passbooks Study GuideNoch keine Bewertungen
- Fundamentals of NursingDokument29 SeitenFundamentals of NursingThierd Cañete IIINoch keine Bewertungen
- INFECTION CONTROL: Passbooks Study GuideVon EverandINFECTION CONTROL: Passbooks Study GuideNoch keine Bewertungen
- Professional Adjustment - KenDokument7 SeitenProfessional Adjustment - KenclobregasNoch keine Bewertungen
- Humanism, Nursing, Communication and Holistic Care: a Position Paper: Position PaperVon EverandHumanism, Nursing, Communication and Holistic Care: a Position Paper: Position PaperNoch keine Bewertungen
- Comhealth NursingDokument58 SeitenComhealth NursingJamil Lorca100% (5)
- The Battle Against Covid-19 Filipino American Healthcare Workers on the Frontlines of the Pandemic ResponseVon EverandThe Battle Against Covid-19 Filipino American Healthcare Workers on the Frontlines of the Pandemic ResponseNoch keine Bewertungen
- Or Illness Were Often Related To Superstitious: Beliefs and The Treatment Also Often Involved Magical CuresDokument29 SeitenOr Illness Were Often Related To Superstitious: Beliefs and The Treatment Also Often Involved Magical CuresMitchee ZialcitaNoch keine Bewertungen
- NURSING EMERGENCIES. 10 BASED TEST QUESTIONS WITH BIBLIOGRAPHYVon EverandNURSING EMERGENCIES. 10 BASED TEST QUESTIONS WITH BIBLIOGRAPHYNoch keine Bewertungen
- Community Health NursingDokument30 SeitenCommunity Health NursingMerrel Ann CNoch keine Bewertungen
- CHN Lecture WCCDokument75 SeitenCHN Lecture WCCMeeKo VideñaNoch keine Bewertungen
- Community Health Nursing PDFDokument25 SeitenCommunity Health Nursing PDFCharles J B. VisayaNoch keine Bewertungen
- Community Focused Nursing: Passbooks Study GuideVon EverandCommunity Focused Nursing: Passbooks Study GuideNoch keine Bewertungen
- Doh MCNDokument14 SeitenDoh MCNCbrc CebuNoch keine Bewertungen
- Nursing Diagnoses 2012-14: Definitions and ClassificationVon EverandNursing Diagnoses 2012-14: Definitions and ClassificationBewertung: 5 von 5 Sternen5/5 (1)
- Community Health NursingDokument78 SeitenCommunity Health NursingJagveer ChauhanNoch keine Bewertungen
- NURSING CARE OF ADULTS II: Passbooks Study GuideVon EverandNURSING CARE OF ADULTS II: Passbooks Study GuideNoch keine Bewertungen
- June 2008 Board Exam TipsDokument5 SeitenJune 2008 Board Exam TipsOnil CallejoNoch keine Bewertungen
- DOH PowerpointDokument232 SeitenDOH PowerpointEmmanuel ApuliNoch keine Bewertungen
- Health & IllnessDokument20 SeitenHealth & IllnessAlessandra Marigold Aguilar Perez100% (1)
- Nutrition 1Dokument6 SeitenNutrition 1jeshemaNoch keine Bewertungen
- My Reviewer On Funda Epaphras Joel T. MilitarDokument82 SeitenMy Reviewer On Funda Epaphras Joel T. MilitarEpaphras Joel MilitarNoch keine Bewertungen
- Sample Nursing Exams-BudekDokument4 SeitenSample Nursing Exams-BudekLj FerolinoNoch keine Bewertungen
- Community Health NursingDokument23 SeitenCommunity Health NursingMimi Vee100% (1)
- Np1 CHN HandoutsDokument61 SeitenNp1 CHN HandoutsRiezah EncisaNoch keine Bewertungen
- Chapter 1 - Health Care Delivery and Nursing PracticeDokument4 SeitenChapter 1 - Health Care Delivery and Nursing Practicejane amosNoch keine Bewertungen
- Compilation of Nursing Theories With Concept AnalyzationDokument164 SeitenCompilation of Nursing Theories With Concept AnalyzationPatrick PantuaNoch keine Bewertungen
- Chapter 19Dokument16 SeitenChapter 19missy23pap100% (1)
- Preoperative Surgical NursngDokument271 SeitenPreoperative Surgical NursngPaw PawNoch keine Bewertungen
- Nle Test Plan For July 2012 Nle: Nursing Practice IDokument7 SeitenNle Test Plan For July 2012 Nle: Nursing Practice IPhilip AdallaNoch keine Bewertungen
- Seminar On Primary Health Care AND Primary Health Centre: Presented By: Ms. Neeta JimmichenDokument99 SeitenSeminar On Primary Health Care AND Primary Health Centre: Presented By: Ms. Neeta JimmichenneetsjimmichenNoch keine Bewertungen
- Professional Adjustment Final 2Dokument41 SeitenProfessional Adjustment Final 2lielani_martinezNoch keine Bewertungen
- Scope of Nle1116aDokument413 SeitenScope of Nle1116aericNoch keine Bewertungen
- 100 Item Exam On Fundamentals of Nursing Keys2Dokument15 Seiten100 Item Exam On Fundamentals of Nursing Keys2Aijem RyanNoch keine Bewertungen
- Nursing As A ProfessionDokument3 SeitenNursing As A ProfessionSHANE VALERIE DIEZNoch keine Bewertungen
- Maternal and Child Health Nursing (NCM 101 Lect) Part 2Dokument2 SeitenMaternal and Child Health Nursing (NCM 101 Lect) Part 2yunjung0518100% (1)
- EPI HandoutDokument8 SeitenEPI HandoutBev YuNoch keine Bewertungen
- CHNDokument340 SeitenCHNPao ParelNoch keine Bewertungen
- Concept of Man and IllnessDokument45 SeitenConcept of Man and IllnessCoronel, Aliene Mea L.Noch keine Bewertungen
- CHN (1) Community Health NursingDokument1 SeiteCHN (1) Community Health NursingImation DataNoch keine Bewertungen
- Fundamentals of Nursing ReviewerDokument31 SeitenFundamentals of Nursing Reviewerbrianwenceslao4100% (3)
- Nursing Review Bullet For Funda (-Credits To OWNER-)Dokument4 SeitenNursing Review Bullet For Funda (-Credits To OWNER-)Camille Honeyleith Lanuza FernandoNoch keine Bewertungen
- Nursing ReviewerDokument11 SeitenNursing ReviewerEllaine JoyceNoch keine Bewertungen
- Board Exam 4Dokument20 SeitenBoard Exam 4Kira100% (9)
- Reviewer For Fundamental of NursingDokument37 SeitenReviewer For Fundamental of NursingtabiNoch keine Bewertungen
- IMCI Chart BookletDokument39 SeitenIMCI Chart Bookletкristina YambaNoch keine Bewertungen
- Nursing Lecture RespiratoryDokument13 SeitenNursing Lecture RespiratoryAedge010100% (1)
- Maternal (Well-Client) : Framework of Maternal and Child CareDokument3 SeitenMaternal (Well-Client) : Framework of Maternal and Child CarealallaallalaNoch keine Bewertungen
- CHN NotesDokument7 SeitenCHN NotesAnvi Turingan PedronanNoch keine Bewertungen
- Practice Test Questions Downloaded From FILIPINO NURSES CENTRALDokument179 SeitenPractice Test Questions Downloaded From FILIPINO NURSES CENTRALFilipino Nurses Central100% (2)
- Preliminary ExaminationDokument58 SeitenPreliminary ExaminationKaycelyn JimenezNoch keine Bewertungen
- Updated - Prioritization of ProblemsDokument1 SeiteUpdated - Prioritization of ProblemsKaycelyn JimenezNoch keine Bewertungen
- Prioritization of ProblemsDokument1 SeitePrioritization of ProblemsKaycelyn JimenezNoch keine Bewertungen
- 199903549Dokument18 Seiten199903549Kaycelyn JimenezNoch keine Bewertungen
- Unsaturated FatDokument4 SeitenUnsaturated FatKaycelyn JimenezNoch keine Bewertungen
- FAMILY Home VisitDokument5 SeitenFAMILY Home VisitKaycelyn JimenezNoch keine Bewertungen
- Minutes of Second English Language Panel Meeting 2023Dokument3 SeitenMinutes of Second English Language Panel Meeting 2023Irwandi Bin Othman100% (1)
- Assignment MS-28 Course Code: MS - 28 Course Title: Labour Laws Assignment Code: MS-28/TMA/SEM - II /2012 Coverage: All BlocksDokument27 SeitenAssignment MS-28 Course Code: MS - 28 Course Title: Labour Laws Assignment Code: MS-28/TMA/SEM - II /2012 Coverage: All BlocksAnjnaKandariNoch keine Bewertungen
- Research ProposalDokument21 SeitenResearch Proposalkecy casamayorNoch keine Bewertungen
- 3rd Periodic Test - Mapeh 9Dokument3 Seiten3rd Periodic Test - Mapeh 9Rap Arante90% (30)
- Engels SEM1 SECONDDokument2 SeitenEngels SEM1 SECONDJolien DeceuninckNoch keine Bewertungen
- People Vs Gonzales-Flores - 138535-38 - April 19, 2001 - JDokument10 SeitenPeople Vs Gonzales-Flores - 138535-38 - April 19, 2001 - JTrexPutiNoch keine Bewertungen
- Deed OfAdjudication Cresencio Abuluyan BasilioDokument4 SeitenDeed OfAdjudication Cresencio Abuluyan BasilioJose BonifacioNoch keine Bewertungen
- Cases in Political Law Review (2nd Batch)Dokument1 SeiteCases in Political Law Review (2nd Batch)Michael Angelo LabradorNoch keine Bewertungen
- CV - Parisi - UChileDokument5 SeitenCV - Parisi - UChileFen_udechileNoch keine Bewertungen
- Wine Express Motion To DismissDokument19 SeitenWine Express Motion To DismissRuss LatinoNoch keine Bewertungen
- Options TraderDokument2 SeitenOptions TraderSoumava PaulNoch keine Bewertungen
- BB 100 - Design For Fire Safety in SchoolsDokument160 SeitenBB 100 - Design For Fire Safety in SchoolsmyscriblkNoch keine Bewertungen
- Sales-Management Solved MCQsDokument69 SeitenSales-Management Solved MCQskrishna100% (3)
- Sri Lskhmi BharatgasDokument2 SeitenSri Lskhmi BharatgasMytreyi AtluriNoch keine Bewertungen
- Catalog - Focus ElectronicDokument14 SeitenCatalog - Focus ElectronicLi KurtNoch keine Bewertungen
- Profil AVANCER FM SERVICES SDN BHDDokument23 SeitenProfil AVANCER FM SERVICES SDN BHDmazhar74Noch keine Bewertungen
- PRCSSPBuyer Can't See Catalog Items While Clicking On Add From Catalog On PO Line (Doc ID 2544576.1 PDFDokument2 SeitenPRCSSPBuyer Can't See Catalog Items While Clicking On Add From Catalog On PO Line (Doc ID 2544576.1 PDFRady KotbNoch keine Bewertungen
- Facilitators of Globalization PresentationDokument3 SeitenFacilitators of Globalization PresentationCleon Roxann WebbeNoch keine Bewertungen
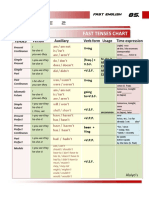
- Table 2: Fast Tenses ChartDokument5 SeitenTable 2: Fast Tenses ChartAngel Julian HernandezNoch keine Bewertungen
- Literature Component SPM'13 Form 4 FullDokument12 SeitenLiterature Component SPM'13 Form 4 FullNur Izzati Abd ShukorNoch keine Bewertungen
- Specific Relief Act, 1963Dokument23 SeitenSpecific Relief Act, 1963Saahiel Sharrma0% (1)
- Discussion: Functions, Advantages and Disadvantages of BIOPOT Cassava Peel and Husk CharcoalDokument4 SeitenDiscussion: Functions, Advantages and Disadvantages of BIOPOT Cassava Peel and Husk CharcoalAhmad BurhanudinNoch keine Bewertungen
- Lord Chief Justice Speech On Jury TrialsDokument10 SeitenLord Chief Justice Speech On Jury TrialsThe GuardianNoch keine Bewertungen
- Memorandum of Inderstanding Ups and GoldcoastDokument3 SeitenMemorandum of Inderstanding Ups and Goldcoastred_21Noch keine Bewertungen
- Design and Pricing of Deposit ServicesDokument37 SeitenDesign and Pricing of Deposit ServicesThe Cultural CommitteeNoch keine Bewertungen
- Statis Pro Park EffectsDokument4 SeitenStatis Pro Park EffectspeppylepepperNoch keine Bewertungen
- 1 s2.0 S0141391023000721 MainDokument28 Seiten1 s2.0 S0141391023000721 MainYemey Quispe ParedesNoch keine Bewertungen
- Transportation Systems ManagementDokument9 SeitenTransportation Systems ManagementSuresh100% (4)
- Mormond History StudyDokument16 SeitenMormond History StudyAndy SturdyNoch keine Bewertungen
- 4th Exam Report - Cabales V CADokument4 Seiten4th Exam Report - Cabales V CAGennard Michael Angelo AngelesNoch keine Bewertungen
- Do You Believe in Magic?: The Sense and Nonsense of Alternative MedicineVon EverandDo You Believe in Magic?: The Sense and Nonsense of Alternative MedicineNoch keine Bewertungen
- Summary: The Myth of Normal: Trauma, Illness, and Healing in a Toxic Culture By Gabor Maté MD & Daniel Maté: Key Takeaways, Summary & AnalysisVon EverandSummary: The Myth of Normal: Trauma, Illness, and Healing in a Toxic Culture By Gabor Maté MD & Daniel Maté: Key Takeaways, Summary & AnalysisBewertung: 4 von 5 Sternen4/5 (9)
- Deaths of Despair and the Future of CapitalismVon EverandDeaths of Despair and the Future of CapitalismBewertung: 4.5 von 5 Sternen4.5/5 (30)
- Uncontrolled Spread: Why COVID-19 Crushed Us and How We Can Defeat the Next PandemicVon EverandUncontrolled Spread: Why COVID-19 Crushed Us and How We Can Defeat the Next PandemicNoch keine Bewertungen
- There Are No Accidents: The Deadly Rise of Injury and Disaster—Who Profits and Who Pays the PriceVon EverandThere Are No Accidents: The Deadly Rise of Injury and Disaster—Who Profits and Who Pays the PriceBewertung: 4.5 von 5 Sternen4.5/5 (15)
- The Truth about Wuhan: How I Uncovered the Biggest Lie in HistoryVon EverandThe Truth about Wuhan: How I Uncovered the Biggest Lie in HistoryBewertung: 4 von 5 Sternen4/5 (6)
- The Gut-Immune Connection: How Understanding the Connection Between Food and Immunity Can Help Us Regain Our HealthVon EverandThe Gut-Immune Connection: How Understanding the Connection Between Food and Immunity Can Help Us Regain Our HealthNoch keine Bewertungen
- The Wisdom of Plagues: Lessons from 25 Years of Covering PandemicsVon EverandThe Wisdom of Plagues: Lessons from 25 Years of Covering PandemicsBewertung: 4.5 von 5 Sternen4.5/5 (6)
- Epic Measures: One Doctor. Seven Billion Patients.Von EverandEpic Measures: One Doctor. Seven Billion Patients.Bewertung: 4 von 5 Sternen4/5 (13)
- Heat Wave: A Social Autopsy of Disaster in ChicagoVon EverandHeat Wave: A Social Autopsy of Disaster in ChicagoBewertung: 4 von 5 Sternen4/5 (40)
- The Inescapable Immune Escape PandemicVon EverandThe Inescapable Immune Escape PandemicBewertung: 5 von 5 Sternen5/5 (1)
- Clean: Overcoming Addiction and Ending America’s Greatest TragedyVon EverandClean: Overcoming Addiction and Ending America’s Greatest TragedyBewertung: 4 von 5 Sternen4/5 (18)
- The Bodies of Others: The New Authoritarians, COVID-19 and The War Against the HumanVon EverandThe Bodies of Others: The New Authoritarians, COVID-19 and The War Against the HumanBewertung: 4.5 von 5 Sternen4.5/5 (12)
- Summary: The Real Anthony Fauci: Bill Gates, Big Pharma, and the Global War on Democracy and Public Health by Robert F. Kennedy Jr: Key Takeaways, Summary & Analysis IncludedVon EverandSummary: The Real Anthony Fauci: Bill Gates, Big Pharma, and the Global War on Democracy and Public Health by Robert F. Kennedy Jr: Key Takeaways, Summary & Analysis IncludedNoch keine Bewertungen
- Profiles of the Vaccine-Injured: "A Lifetime Price to Pay"Von EverandProfiles of the Vaccine-Injured: "A Lifetime Price to Pay"Bewertung: 3.5 von 5 Sternen3.5/5 (3)
- Sickening: How Big Pharma Broke American Health Care and How We Can Repair ItVon EverandSickening: How Big Pharma Broke American Health Care and How We Can Repair ItBewertung: 4 von 5 Sternen4/5 (9)
- The Wuhan Cover-Up: And the Terrifying Bioweapons Arms RaceVon EverandThe Wuhan Cover-Up: And the Terrifying Bioweapons Arms RaceNoch keine Bewertungen
- Get Well Soon: History's Worst Plagues and the Heroes Who Fought ThemVon EverandGet Well Soon: History's Worst Plagues and the Heroes Who Fought ThemBewertung: 4 von 5 Sternen4/5 (234)
- Fatal Conveniences: The Toxic Products and Harmful Habits That Are Making You Sick—and the Simple Changes That Will Save Your HealthVon EverandFatal Conveniences: The Toxic Products and Harmful Habits That Are Making You Sick—and the Simple Changes That Will Save Your HealthBewertung: 4 von 5 Sternen4/5 (7)
- Vaccines Did Not Cause Rachel's Autism: My Journey as a Vaccine Scientist, Pediatrician, and Autism DadVon EverandVaccines Did Not Cause Rachel's Autism: My Journey as a Vaccine Scientist, Pediatrician, and Autism DadBewertung: 4.5 von 5 Sternen4.5/5 (3)
- There Are No Accidents: The Deadly Rise of Injury and Disaster—Who Profits and Who Pays the PriceVon EverandThere Are No Accidents: The Deadly Rise of Injury and Disaster—Who Profits and Who Pays the PriceBewertung: 4.5 von 5 Sternen4.5/5 (11)
- The Price of Health: The Modern Pharmaceutical Enterprise and the Betrayal of a History of CareVon EverandThe Price of Health: The Modern Pharmaceutical Enterprise and the Betrayal of a History of CareNoch keine Bewertungen
- Breaking out of the Health Care Abyss: Transformational Tips for Agents of ChangeVon EverandBreaking out of the Health Care Abyss: Transformational Tips for Agents of ChangeNoch keine Bewertungen
- Mama Might Be Better Off Dead: The Failure of Health Care in Urban AmericaVon EverandMama Might Be Better Off Dead: The Failure of Health Care in Urban AmericaNoch keine Bewertungen
- Environmental Health and Occupational Health & SafetyVon EverandEnvironmental Health and Occupational Health & SafetyBewertung: 3.5 von 5 Sternen3.5/5 (9)