Das könnte Ihnen auch gefallen
- Neurology NotesDokument87 SeitenNeurology Notessuggaplum100% (2)
- Neurologic AssessmentDokument8 SeitenNeurologic AssessmentHNoch keine Bewertungen
- Introductory Herbal Course Outline by the Herbal AcademyDokument6 SeitenIntroductory Herbal Course Outline by the Herbal AcademyErick Lopez100% (2)
- 2016 January FebruaryDokument45 Seiten2016 January FebruaryAndriusjo100% (1)
- Pediatric History and Physical Exam GuideDokument7 SeitenPediatric History and Physical Exam GuideIndunil AnuruddhikaNoch keine Bewertungen
- Guide to Evaluating and Diagnosing Common Headache DisordersDokument54 SeitenGuide to Evaluating and Diagnosing Common Headache DisorderssaharuiNoch keine Bewertungen
- Active Listening HANDOUT PDFDokument26 SeitenActive Listening HANDOUT PDFMiguel Cuevas DolotNoch keine Bewertungen
- Get A New Client Today FinalDokument22 SeitenGet A New Client Today FinalValaki Aki100% (1)
- Neurology Multiple Choice Questions With Explanations: Volume IIVon EverandNeurology Multiple Choice Questions With Explanations: Volume IIBewertung: 5 von 5 Sternen5/5 (2)
- Headache: Thomas Kwiatkowski and Kumar AlagappanDokument11 SeitenHeadache: Thomas Kwiatkowski and Kumar AlagappanS100% (1)
- Community-Acquired Pneumonia - CPG 2016Dokument26 SeitenCommunity-Acquired Pneumonia - CPG 2016Jamie SebastianNoch keine Bewertungen
- Australian Ironman Magazine July 2016 PDFDokument140 SeitenAustralian Ironman Magazine July 2016 PDFgeorgeNoch keine Bewertungen
- Causes and Tests of Upper Cervical Spine PainDokument22 SeitenCauses and Tests of Upper Cervical Spine PainiikemNoch keine Bewertungen
- 3 Drugs Study Updates Issues HemodialysisDokument7 Seiten3 Drugs Study Updates Issues HemodialysisKim GalamgamNoch keine Bewertungen
- An Introduction To Basic Medical English Terminology 1Dokument346 SeitenAn Introduction To Basic Medical English Terminology 1bbbanyi100% (2)
- NCM 100 SKILLS Nursing Process HandoutsDokument10 SeitenNCM 100 SKILLS Nursing Process HandoutsPearl IbisateNoch keine Bewertungen
- Anesthesia Pocket Cards 7 18 18Dokument6 SeitenAnesthesia Pocket Cards 7 18 18Miguel Cuevas DolotNoch keine Bewertungen
- Neurological DisordersDokument20 SeitenNeurological DisordersEdil M JamaNoch keine Bewertungen
- HEADACHEDokument12 SeitenHEADACHEAndreas Bobola Abie0% (1)
- Migraine Migraine Migraine Migraine: History of Presenting IllnessDokument22 SeitenMigraine Migraine Migraine Migraine: History of Presenting IllnessTom MallinsonNoch keine Bewertungen
- Effectiveness of Transdermal MagnesiumDokument2 SeitenEffectiveness of Transdermal MagnesiumMiguel Cuevas Dolot100% (1)
- Initial Thesis Report (Global Ayurvedic Village)Dokument26 SeitenInitial Thesis Report (Global Ayurvedic Village)dipu singh82% (11)
- Inserting A Nasogastric TubeDokument5 SeitenInserting A Nasogastric TubeWendy EscalanteNoch keine Bewertungen
- Primary Headache in Clinical PracticeDokument68 SeitenPrimary Headache in Clinical PracticeAkbar RasyidsonyNoch keine Bewertungen
- Anatomy of KidneyDokument3 SeitenAnatomy of KidneyjibbyNoch keine Bewertungen
- Primary Headache DisordersDokument5 SeitenPrimary Headache DisordersEarle NiervoNoch keine Bewertungen
- Chronic Headache: DR Maziah BT Ishak DR Sharifah Amirah BT Syed Abd - HamidDokument30 SeitenChronic Headache: DR Maziah BT Ishak DR Sharifah Amirah BT Syed Abd - HamidSueNoch keine Bewertungen
- Internal Medicine 2 - Nasir VersionDokument55 SeitenInternal Medicine 2 - Nasir VersionAhmad SobihNoch keine Bewertungen
- 2.2CDPDHeadacheVISIONDokument7 Seiten2.2CDPDHeadacheVISIONEduardo Marco Villarama DayritNoch keine Bewertungen
- NCM118 TransesDokument11 SeitenNCM118 TransesAlejandro Saclolo, IIINoch keine Bewertungen
- Step 2 CS - Headache DDX, Physical Exam, Work-UpDokument118 SeitenStep 2 CS - Headache DDX, Physical Exam, Work-UpnaimNoch keine Bewertungen
- Headche:Dizzy Med Stud - 2016Dokument51 SeitenHeadche:Dizzy Med Stud - 2016Surat TanprawateNoch keine Bewertungen
- Headache Barja Edited 1Dokument8 SeitenHeadache Barja Edited 1Eduardo Marco Villarama DayritNoch keine Bewertungen
- Postpartum Headache: Diagnostic Considerations: Sue Yin Lim, Nikos Evangelou, Sibylle JürgensDokument8 SeitenPostpartum Headache: Diagnostic Considerations: Sue Yin Lim, Nikos Evangelou, Sibylle JürgensJamie LittleNoch keine Bewertungen
- Headache: Red FlagsDokument1 SeiteHeadache: Red FlagsNadia SalwaniNoch keine Bewertungen
- Headache in Neurological EmergencyDokument8 SeitenHeadache in Neurological EmergencyJorge Andres Restrepo VillaNoch keine Bewertungen
- Admitting Conference: Abejo, Jerika D. Bona, Henry JR.Dokument38 SeitenAdmitting Conference: Abejo, Jerika D. Bona, Henry JR.Henry BonaNoch keine Bewertungen
- UntitledDokument28 SeitenUntitledAbdalla esayedNoch keine Bewertungen
- Meded Emq Revision Course Notes Set 1Dokument44 SeitenMeded Emq Revision Course Notes Set 1py siraNoch keine Bewertungen
- Vertebral Artery DissectionDokument2 SeitenVertebral Artery DissectionTom MallinsonNoch keine Bewertungen
- Blumenfeld Neuroanatomy Ch. 5 SummaryDokument5 SeitenBlumenfeld Neuroanatomy Ch. 5 SummaryMeeraNoch keine Bewertungen
- Neurosurgery ReportingDokument63 SeitenNeurosurgery ReportingMa. Jessa Victoria VallangcaNoch keine Bewertungen
- Subarachnoid HemorrhageDokument2 SeitenSubarachnoid Hemorrhagevfsqp9zxgqNoch keine Bewertungen
- Acute Headache: Raeburn B. ForbesDokument7 SeitenAcute Headache: Raeburn B. ForbesAnonymous nruHyuwtJNoch keine Bewertungen
- Department of Family Medicine Fpe Headache Syndrome: - Vanaveera Pandian SwethaDokument106 SeitenDepartment of Family Medicine Fpe Headache Syndrome: - Vanaveera Pandian SwethaSuba Saravanan 12Noch keine Bewertungen
- NeurologyDokument42 SeitenNeurologyPierre BenardNoch keine Bewertungen
- Headache - Migraine: Dr.S.Pranavendra Nath, Junior Resident, Dept. of Internal Medicine, Kims & RFDokument62 SeitenHeadache - Migraine: Dr.S.Pranavendra Nath, Junior Resident, Dept. of Internal Medicine, Kims & RFpurnaNoch keine Bewertungen
- Headache NotesDokument25 SeitenHeadache NotesAin AmanyNoch keine Bewertungen
- Pediatric NursingDokument14 SeitenPediatric NursingJoanne PaulineNoch keine Bewertungen
- Headache Types and CausesDokument6 SeitenHeadache Types and Causes3BBEGILJUDY ANNBNoch keine Bewertungen
- Headache ReviewDokument8 SeitenHeadache Reviewoscar nieblesNoch keine Bewertungen
- HeadacheDokument3 SeitenHeadacheanime listNoch keine Bewertungen
- StrokeDokument27 SeitenStrokeJASON KO CHIA SHENGNoch keine Bewertungen
- Neurology - : Approach To Headache DisordersDokument8 SeitenNeurology - : Approach To Headache DisordersKarenNoch keine Bewertungen
- Cefalea y AneurismaDokument6 SeitenCefalea y AneurismaJesús Evangelista GomerNoch keine Bewertungen
- Nyeri Kepala (Sefalgia) : Luhu A. Tapiheru Fakultas Kedokteran Umsu MedanDokument108 SeitenNyeri Kepala (Sefalgia) : Luhu A. Tapiheru Fakultas Kedokteran Umsu MedanLestari Amelia AdmNoch keine Bewertungen
- Koma dan Penurunan KesadaranDokument40 SeitenKoma dan Penurunan KesadaranAhmad Shafwan NatsirNoch keine Bewertungen
- Common Neuromuscular DiseasesDokument4 SeitenCommon Neuromuscular DiseasesRitz CelsoNoch keine Bewertungen
- Stroke, Meningitis, Parkinson's, and Bell's Palsy Guide for NursesDokument2 SeitenStroke, Meningitis, Parkinson's, and Bell's Palsy Guide for NursesHeather Wray-WilsonNoch keine Bewertungen
- Nervous System Disorders Lecture Notes 6 - 7 - 20Dokument31 SeitenNervous System Disorders Lecture Notes 6 - 7 - 20Cynthia FloresNoch keine Bewertungen
- Understanding Headaches: Causes, Symptoms and TreatmentDokument40 SeitenUnderstanding Headaches: Causes, Symptoms and TreatmentJoni Lyn Ba-as BayengNoch keine Bewertungen
- Understanding Pain Pathways and Headache CausesDokument219 SeitenUnderstanding Pain Pathways and Headache CausesBiman MondalNoch keine Bewertungen
- IPD A Cardiovascular System Bates and and VideoDokument10 SeitenIPD A Cardiovascular System Bates and and Videostar220498Noch keine Bewertungen
- LAPORAN CASE V HEADACHE AND PAINDokument43 SeitenLAPORAN CASE V HEADACHE AND PAINMochamadFirdausNoch keine Bewertungen
- Headache: Setyawati Asih PutriDokument79 SeitenHeadache: Setyawati Asih PutriAngga FirmansyahNoch keine Bewertungen
- Increased ICP and Neurological Trauma GuideDokument14 SeitenIncreased ICP and Neurological Trauma GuideMhoy CostesNoch keine Bewertungen
- Head Injury Diagnosis and ManagementDokument41 SeitenHead Injury Diagnosis and ManagementChristian Dave EndinoNoch keine Bewertungen
- Updated Headache 21-22Dokument48 SeitenUpdated Headache 21-22jwxxi11Noch keine Bewertungen
- NeurologyDokument91 SeitenNeurologyjaffar mahNoch keine Bewertungen
- Disease Comparison ChartDokument36 SeitenDisease Comparison ChartSara S. CastañedaNoch keine Bewertungen
- Neurological SheetDokument70 SeitenNeurological Sheetdrprasant100% (6)
- QuizletDokument37 SeitenQuizletnaimNoch keine Bewertungen
- Headache PAINDokument1 SeiteHeadache PAINOmarNoch keine Bewertungen
- Trigeminal Nerve Pain: A Guide to Clinical ManagementVon EverandTrigeminal Nerve Pain: A Guide to Clinical ManagementAlaa Abd-ElsayedNoch keine Bewertungen
- Covid 19 CPR 7 RulesDokument21 SeitenCovid 19 CPR 7 RulesMiguel Cuevas DolotNoch keine Bewertungen
- PSB 368Dokument6 SeitenPSB 368Miguel Cuevas DolotNoch keine Bewertungen
- Covid 19 CPR 7 RulesDokument21 SeitenCovid 19 CPR 7 RulesMiguel Cuevas DolotNoch keine Bewertungen
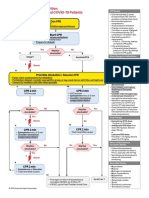
- ACLS Cardiac Arrest Algorithm For Suspected or Confirmed COVID-19 PatientsDokument1 SeiteACLS Cardiac Arrest Algorithm For Suspected or Confirmed COVID-19 PatientsMariuxi Tatiana ChocoNoch keine Bewertungen
- Physical Examination in ENT: Ussana Promyothin, MDDokument60 SeitenPhysical Examination in ENT: Ussana Promyothin, MDMiguel Cuevas DolotNoch keine Bewertungen
- Clinical Examination of The Ear, Nose and Throat: Dave Pothier ST Mary's 2003Dokument30 SeitenClinical Examination of The Ear, Nose and Throat: Dave Pothier ST Mary's 2003Ekambaram TrmNoch keine Bewertungen
- (MED) COVID-19 Trans V. 2.0Dokument6 Seiten(MED) COVID-19 Trans V. 2.0Isabel VinasNoch keine Bewertungen
- Physical Assessment: Ear, Nose, Mouth, and ThroatDokument59 SeitenPhysical Assessment: Ear, Nose, Mouth, and ThroatMiguel Cuevas DolotNoch keine Bewertungen
- How Can Patients Visitors Help - May18Dokument2 SeitenHow Can Patients Visitors Help - May18Miguel Cuevas DolotNoch keine Bewertungen
- Vertigo Gail Ishiyama 1 13 10Dokument40 SeitenVertigo Gail Ishiyama 1 13 10Myname Rama LienNoch keine Bewertungen
- Physical Examination in ENT: Ussana Promyothin, MDDokument60 SeitenPhysical Examination in ENT: Ussana Promyothin, MDMiguel Cuevas DolotNoch keine Bewertungen
- Covid 19 PDFDokument18 SeitenCovid 19 PDFMiguel Cuevas DolotNoch keine Bewertungen
- Cook Book (Filipino) 13 PDFDokument23 SeitenCook Book (Filipino) 13 PDFAdina AnghelNoch keine Bewertungen
- Benign Paroxysmal Positional Vertigo: Waseem WatadDokument37 SeitenBenign Paroxysmal Positional Vertigo: Waseem WatadnoviNoch keine Bewertungen
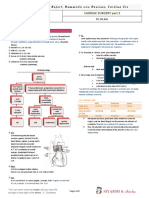
- TCVS - Cardiac Surgery Part 2 Dr. de AsisDokument8 SeitenTCVS - Cardiac Surgery Part 2 Dr. de AsisMiguel Cuevas DolotNoch keine Bewertungen
- Pedia Tickler Update 2017Dokument2 SeitenPedia Tickler Update 2017Tani BokNoch keine Bewertungen
- Clinical AbstractDokument4 SeitenClinical AbstractMiguel Cuevas DolotNoch keine Bewertungen
- A Case-Control Study of The Association of Diet and Obesity With Gout in Taiwan PDFDokument12 SeitenA Case-Control Study of The Association of Diet and Obesity With Gout in Taiwan PDFMiguel Cuevas DolotNoch keine Bewertungen
- A Case-Control Study of The Association of Diet and Obesity With Gout in Taiwan PDFDokument12 SeitenA Case-Control Study of The Association of Diet and Obesity With Gout in Taiwan PDFMiguel Cuevas DolotNoch keine Bewertungen
- Nocturnals Physiology 2018Dokument14 SeitenNocturnals Physiology 2018Miguel Cuevas DolotNoch keine Bewertungen
- Drug IndexDokument2 SeitenDrug IndexMiguel Cuevas DolotNoch keine Bewertungen
- HEMAreviewDokument3 SeitenHEMAreviewMiguel Cuevas DolotNoch keine Bewertungen
- Neurologic ExamDokument1 SeiteNeurologic ExamMiguel Cuevas DolotNoch keine Bewertungen
- Kerosene PDFDokument31 SeitenKerosene PDFRudyMLanaNoch keine Bewertungen
- European Jr. Cancer 160 2022Dokument37 SeitenEuropean Jr. Cancer 160 2022cdsaludNoch keine Bewertungen
- PHRM TemplateDokument4 SeitenPHRM TemplateRichard SakyiamahNoch keine Bewertungen
- (FREE SAMPLE) The Performance Digest - Issue 17 (March 18)Dokument45 Seiten(FREE SAMPLE) The Performance Digest - Issue 17 (March 18)Giovanni SlackNoch keine Bewertungen
- Freud Och Moreno - A ComparisonDokument33 SeitenFreud Och Moreno - A ComparisonLarsTauvon100% (2)
- Trial 2Dokument2 SeitenTrial 2Jayzelle Anne de LeonNoch keine Bewertungen
- Fornas RS MataDokument12 SeitenFornas RS MataHery SatriawanNoch keine Bewertungen
- Anticonvulsant Anti-Epileptic Uwolfia Alkaloids: Action of Some Drugs Mice Pre-Treated WithDokument6 SeitenAnticonvulsant Anti-Epileptic Uwolfia Alkaloids: Action of Some Drugs Mice Pre-Treated WithAwanish MishraNoch keine Bewertungen
- Bridging For Patients On DOACs/NOACsDokument1 SeiteBridging For Patients On DOACs/NOACsZieshNoch keine Bewertungen
- Active PackagingDokument27 SeitenActive PackagingKartika Sari SubagioNoch keine Bewertungen
- WL DeterminationDokument12 SeitenWL Determinationdr asiyaNoch keine Bewertungen
- Copd19 PDFDokument31 SeitenCopd19 PDFAdinda Suci MaghfiraNoch keine Bewertungen
- Coffea - The Best Homeopathic Medicine For Insomnia: Insomnia Treatment in HomeopathyDokument4 SeitenCoffea - The Best Homeopathic Medicine For Insomnia: Insomnia Treatment in HomeopathysharmadxNoch keine Bewertungen
- Glasgow Coma Scale and Causes of ComaDokument6 SeitenGlasgow Coma Scale and Causes of ComaEm Hernandez AranaNoch keine Bewertungen
- Costochondritis - Causes, Symptoms and Treatment - by Owen Jones - MediumDokument1 SeiteCostochondritis - Causes, Symptoms and Treatment - by Owen Jones - MediumkamrevariNoch keine Bewertungen
- Daftar PustakaDokument2 SeitenDaftar PustakaMuhammad Andika Ekaputra RianilNoch keine Bewertungen
- Stok All-18Dokument24 SeitenStok All-18apotekindomedispkyNoch keine Bewertungen
- Pre - Operative SurgeryDokument3 SeitenPre - Operative SurgeryFan Eli100% (5)
- Coughlin CC Case Study IntroDokument3 SeitenCoughlin CC Case Study Introapi-283315953100% (1)
- Management of Pancreatic Calculi: An Update: ReviewDokument8 SeitenManagement of Pancreatic Calculi: An Update: ReviewFarid RakhmanNoch keine Bewertungen
- Dengue Discharge PlanDokument1 SeiteDengue Discharge PlanChris Denver BancaleNoch keine Bewertungen
- Cluster 5: Written Assignment: Before Completing and Submitting This Assignment, Have You: What You Have To DoDokument10 SeitenCluster 5: Written Assignment: Before Completing and Submitting This Assignment, Have You: What You Have To Dorishabhk28995100% (1)