Das könnte Ihnen auch gefallen
- 5 Membrane Function-SDokument5 Seiten5 Membrane Function-SLeo DingNoch keine Bewertungen
- Johannes Gerbes, Frauke Van Der Werff - Fit Fürs Goethe-Zertifikat, A2 - Start Deutsch 2, Volume 2 (2007, Hueber Verlag)Dokument33 SeitenJohannes Gerbes, Frauke Van Der Werff - Fit Fürs Goethe-Zertifikat, A2 - Start Deutsch 2, Volume 2 (2007, Hueber Verlag)kareemNoch keine Bewertungen
- Biochem. Chapter 7 Notes. Myoglobin and Hemoglobin, Muscle Contraction, and AntibodiesDokument10 SeitenBiochem. Chapter 7 Notes. Myoglobin and Hemoglobin, Muscle Contraction, and AntibodiesOANoch keine Bewertungen
- Chapter 24 Oxygen Toxicity and Hyper 2017 Nunn S Applied Respiratory PhysiDokument18 SeitenChapter 24 Oxygen Toxicity and Hyper 2017 Nunn S Applied Respiratory PhysiFontecha AnaNoch keine Bewertungen
- GR 7 Ventures PEDokument232 SeitenGR 7 Ventures PEFaithNoch keine Bewertungen
- Human Body Systems-Powerpoint Rubric-New 1Dokument4 SeitenHuman Body Systems-Powerpoint Rubric-New 1api-269791459Noch keine Bewertungen
- Hematology Review NotesDokument28 SeitenHematology Review NoteszachNoch keine Bewertungen
- Hematology NCLEX MCQDokument24 SeitenHematology NCLEX MCQKo Ye100% (2)
- Lecture 4 Gas Transport AIU 2022Dokument32 SeitenLecture 4 Gas Transport AIU 2022marwan hagrassNoch keine Bewertungen
- 09 Oxygen CurvesDokument3 Seiten09 Oxygen Curvesramloghun veerNoch keine Bewertungen
- Respiratory Membrane and Transport of OxygenDokument29 SeitenRespiratory Membrane and Transport of OxygenAhmad KhanNoch keine Bewertungen
- Oxygen Transport JOHN W. BAYNES, MAREK H. DOMINICZAK - Medical Biochemistry-Elsevier Inc. (2019)Dokument15 SeitenOxygen Transport JOHN W. BAYNES, MAREK H. DOMINICZAK - Medical Biochemistry-Elsevier Inc. (2019)Malika MohNoch keine Bewertungen
- UAS Kritis 1 (T4) - Monitoring Fungsi Pernapasan - Bu HY (A11)Dokument108 SeitenUAS Kritis 1 (T4) - Monitoring Fungsi Pernapasan - Bu HY (A11)rifqifuadiNoch keine Bewertungen
- Delivering Oxygen: 10.1 Oxygen Is Continually NeededDokument29 SeitenDelivering Oxygen: 10.1 Oxygen Is Continually NeededThomas JoseNoch keine Bewertungen
- O2 Transport CostanzoDokument10 SeitenO2 Transport CostanzoStudent1010Noch keine Bewertungen
- Gas Transport in Blood PPT 1Dokument34 SeitenGas Transport in Blood PPT 1CLEMENTNoch keine Bewertungen
- Oxygen Delivery and ConsumptionDokument2 SeitenOxygen Delivery and ConsumptionAde YonataNoch keine Bewertungen
- DPN-Biochem I - Lecture 8 - Myoglobin and HemoglobinDokument41 SeitenDPN-Biochem I - Lecture 8 - Myoglobin and Hemoglobinchienyu2002Noch keine Bewertungen
- Oxygendissociationcurve 170720115931Dokument60 SeitenOxygendissociationcurve 170720115931Pinky RanwaNoch keine Bewertungen
- Small Animal Oxygen TherapyDokument10 SeitenSmall Animal Oxygen Therapytaner_soysuren100% (1)
- Chapter 9 The Respiratory SystemDokument56 SeitenChapter 9 The Respiratory SystemNurarief AffendyNoch keine Bewertungen
- Transport of Oxygen and Carbon DioxideDokument30 SeitenTransport of Oxygen and Carbon DioxideashwinaaNoch keine Bewertungen
- Chapter 6 Hypoxia: Guo WeiDokument63 SeitenChapter 6 Hypoxia: Guo WeiShourav SarkarNoch keine Bewertungen
- Oxygen Transport by HemoglobinDokument27 SeitenOxygen Transport by HemoglobinLola RojasNoch keine Bewertungen
- Physeo - Lecture 3Dokument21 SeitenPhyseo - Lecture 3Mahmoud hilmyNoch keine Bewertungen
- Transport of GasesDokument39 SeitenTransport of GasesJayballabh KumarNoch keine Bewertungen
- Respiratory Physiology Part 2Dokument5 SeitenRespiratory Physiology Part 2kabir musa ladanNoch keine Bewertungen
- Subject ChemistryDokument12 SeitenSubject ChemistrykottooranjohnbNoch keine Bewertungen
- Lecture 6 Gas TransportDokument37 SeitenLecture 6 Gas Transport7mb767gqyvNoch keine Bewertungen
- Abstrak: 1 - Fakultas Kedokteran UKRIDA - Blok 7: Respiratory 1Dokument9 SeitenAbstrak: 1 - Fakultas Kedokteran UKRIDA - Blok 7: Respiratory 1TreitzNoch keine Bewertungen
- 2022.01.07 Live Session Article EquilibriumDokument4 Seiten2022.01.07 Live Session Article EquilibriumInês AlmeidaNoch keine Bewertungen
- Transport of Oxygen and Carbon DioxideDokument22 SeitenTransport of Oxygen and Carbon DioxideAiza AyazNoch keine Bewertungen
- Biochem PresentationDokument16 SeitenBiochem PresentationRushana SadaqatNoch keine Bewertungen
- Transport of Oxygen and Carbon DioxideDokument22 SeitenTransport of Oxygen and Carbon DioxideSajid Nadaf100% (1)
- Oxigen Oter ApiaDokument16 SeitenOxigen Oter ApiaDiana CarolinaNoch keine Bewertungen
- Bohr EffectDokument22 SeitenBohr EffectFITHANoch keine Bewertungen
- Lec 7 2009 Blood Gas TransportDokument9 SeitenLec 7 2009 Blood Gas TransportAmrutha DasariNoch keine Bewertungen
- Gas Transport 2Dokument29 SeitenGas Transport 2Charmaine LucNoch keine Bewertungen
- Transport of Oxygen and Carbon Dioxide-PartialDokument24 SeitenTransport of Oxygen and Carbon Dioxide-PartialMarie PetalcorinNoch keine Bewertungen
- Physiology of Oxygen Transport and Its Determinants in Intensive Care UnitDokument6 SeitenPhysiology of Oxygen Transport and Its Determinants in Intensive Care UnitHanh NguyenNoch keine Bewertungen
- Transportation of OxygenDokument37 SeitenTransportation of OxygenDrAbhilasha SharmaNoch keine Bewertungen
- 232 Respiratory Physiology External Respiration Partial PressuresDokument3 Seiten232 Respiratory Physiology External Respiration Partial PressuresAhmed JabbarNoch keine Bewertungen
- Blood Groups and TrasnfusionDokument12 SeitenBlood Groups and Trasnfusiondeput_rprNoch keine Bewertungen
- Oxygen Dissociation CurvesDokument3 SeitenOxygen Dissociation Curveslastjoe71100% (1)
- L3 DR Jehad Lect3 Notes RSDokument4 SeitenL3 DR Jehad Lect3 Notes RSBikash chutiaNoch keine Bewertungen
- Gas Exchange & O2 TransportDokument11 SeitenGas Exchange & O2 Transportmina mounirNoch keine Bewertungen
- Gas Exchange - Respirasi Blok 2.1.maret.15Dokument29 SeitenGas Exchange - Respirasi Blok 2.1.maret.15Fatiha TamadNoch keine Bewertungen
- Factors Regulating BreathingDokument15 SeitenFactors Regulating BreathingShubha DiwakarNoch keine Bewertungen
- Pulmonary Presentation MERGEDDokument20 SeitenPulmonary Presentation MERGEDShubha DiwakarNoch keine Bewertungen
- Hemoglobin 150424133422 Conversion Gate01Dokument50 SeitenHemoglobin 150424133422 Conversion Gate01MarcelliaNoch keine Bewertungen
- CaseDokument118 SeitenCaseHendy MasjayantoNoch keine Bewertungen
- Physiology of Oxygen TransportDokument8 SeitenPhysiology of Oxygen TransportAldo FebrianNoch keine Bewertungen
- C7 (Gaseous Exchange)Dokument16 SeitenC7 (Gaseous Exchange)nurhasinahabrahimNoch keine Bewertungen
- Cardiovascular PhysiologyDokument10 SeitenCardiovascular PhysiologyBookwormNoch keine Bewertungen
- HIS 6 - Haemoglobin Recall Oxygen Binding Properties of HB: Iron (II) - Protoporphyrin IXDokument2 SeitenHIS 6 - Haemoglobin Recall Oxygen Binding Properties of HB: Iron (II) - Protoporphyrin IXKristin DouglasNoch keine Bewertungen
- Respiratory PhysiologyDokument45 SeitenRespiratory PhysiologyJohn Christopher LucesNoch keine Bewertungen
- Gas Dalam DarahDokument31 SeitenGas Dalam DarahAndwitya PrameshwariNoch keine Bewertungen
- Gaseous Exchange in HumansDokument21 SeitenGaseous Exchange in Humansaini azzahraNoch keine Bewertungen
- Oxygen Transport - Regulation of Tissue OxygenationDokument2 SeitenOxygen Transport - Regulation of Tissue OxygenationdikshaNoch keine Bewertungen
- L11 Hemoglobin Structure-FunctionDokument26 SeitenL11 Hemoglobin Structure-Functionziyad khalidNoch keine Bewertungen
- From The Atmosphere To The Mitochondrion: The Oxygen CascadeDokument28 SeitenFrom The Atmosphere To The Mitochondrion: The Oxygen CascadeMelisa Martínez HernándezNoch keine Bewertungen
- Guyton and Hall Chapter 40Dokument2 SeitenGuyton and Hall Chapter 40Richelle Dianne Ramos-GiangNoch keine Bewertungen
- Handbook of Coordination Catalysis in Organic ChemistryVon EverandHandbook of Coordination Catalysis in Organic ChemistryNoch keine Bewertungen
- FullDokument6 SeitenFullgerginNoch keine Bewertungen
- Histology: Tissues of The BodyDokument166 SeitenHistology: Tissues of The BodygerginNoch keine Bewertungen
- Sertoli 1Dokument38 SeitenSertoli 1gerginNoch keine Bewertungen
- "The Basics" - Origins of The Integumentary SystemDokument4 Seiten"The Basics" - Origins of The Integumentary SystemgerginNoch keine Bewertungen
- The Immunology of SkinDokument4 SeitenThe Immunology of SkingerginNoch keine Bewertungen
- The Following Notes Are References According To Figures and Tables in Gartner and Hiatt (2 Edition, 2001)Dokument5 SeitenThe Following Notes Are References According To Figures and Tables in Gartner and Hiatt (2 Edition, 2001)gerginNoch keine Bewertungen
- Keratinocyte Maturation Can Be Divided Into Five SequencesDokument5 SeitenKeratinocyte Maturation Can Be Divided Into Five SequencesgerginNoch keine Bewertungen
- Histology of Blood Histology of Blood VesselsDokument6 SeitenHistology of Blood Histology of Blood VesselsgerginNoch keine Bewertungen
- Pituitary, Adrenal, & Thyroid GlandsDokument41 SeitenPituitary, Adrenal, & Thyroid GlandsgerginNoch keine Bewertungen
- Were Dinosaurs Warm Blooded? or Were They Cold Blooded? Does It Really Matter?Dokument11 SeitenWere Dinosaurs Warm Blooded? or Were They Cold Blooded? Does It Really Matter?gerginNoch keine Bewertungen
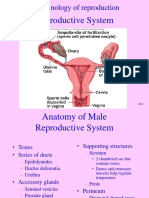
- Reproductive System: Endocrinology of ReproductionDokument40 SeitenReproductive System: Endocrinology of ReproductiongerginNoch keine Bewertungen
- UrogenitalDokument36 SeitenUrogenitalCharlene Chin SeeNoch keine Bewertungen
- Why Catecholamines?: March 29, 2004 Lenore PriceDokument4 SeitenWhy Catecholamines?: March 29, 2004 Lenore PricegerginNoch keine Bewertungen
- Concept MapDokument1 SeiteConcept Mapapi-249598813Noch keine Bewertungen
- Micro HSB A - Myeloid Tissue HistologyDokument2 SeitenMicro HSB A - Myeloid Tissue HistologyGaelle Lisette MacatangayNoch keine Bewertungen
- Listening Script FullDokument93 SeitenListening Script FullkbalvinNoch keine Bewertungen
- Biology Questions For Form Five Students That Can Lead For Their Excel in SPMDokument14 SeitenBiology Questions For Form Five Students That Can Lead For Their Excel in SPMZati Mohd RazibNoch keine Bewertungen
- Lahore Lab: Web ReportDokument1 SeiteLahore Lab: Web Reportkhurram shahzadNoch keine Bewertungen
- Pentra 80 Technical Manual (Internet) PDFDokument333 SeitenPentra 80 Technical Manual (Internet) PDFLuis Raul Soto Marentes100% (4)
- Low Abnormal Control Assayed - 0020003210: ENGLISH - Insert Revision 04/2019Dokument3 SeitenLow Abnormal Control Assayed - 0020003210: ENGLISH - Insert Revision 04/2019Brady AndersonNoch keine Bewertungen
- Anemia Pathophysiology by Francis Oliveros, BSN 4Dokument2 SeitenAnemia Pathophysiology by Francis Oliveros, BSN 4francis00090100% (1)
- An Scie Report Final1Dokument5 SeitenAn Scie Report Final1Abas S. AcmadNoch keine Bewertungen
- Some Questions May Have Been Altered or Removed Compared To The Version of This Paper Used During The Competition Period. Answers Are Not Provided at This TimeDokument41 SeitenSome Questions May Have Been Altered or Removed Compared To The Version of This Paper Used During The Competition Period. Answers Are Not Provided at This TimeFabian “TheLeviathan”Noch keine Bewertungen
- Hematology 2 Topic 2 Prelim2222Dokument73 SeitenHematology 2 Topic 2 Prelim2222Mary Lyka ReyesNoch keine Bewertungen
- Nutriflex Lipid Peri PDFDokument2 SeitenNutriflex Lipid Peri PDFSanjaya FaisalNoch keine Bewertungen
- Minerals ChartDokument2 SeitenMinerals Chartautumn15_7Noch keine Bewertungen
- BIO 220 Fall 2014revDokument5 SeitenBIO 220 Fall 2014revPG0423Noch keine Bewertungen
- 01 - Animal Diversity-I (Theory) PDFDokument51 Seiten01 - Animal Diversity-I (Theory) PDFRohit rajNoch keine Bewertungen
- Managing Clinical Laboratories: Monitor and Control Lab Errors To Improve Lab PerformanceDokument42 SeitenManaging Clinical Laboratories: Monitor and Control Lab Errors To Improve Lab PerformanceRamadhan OlongNoch keine Bewertungen
- Arterial and Venous Pressure Monitoring During Hemodialysis - Document - Gale Academic OneFileDokument10 SeitenArterial and Venous Pressure Monitoring During Hemodialysis - Document - Gale Academic OneFileBryan FarrelNoch keine Bewertungen
- Yin Yang PrimerDokument53 SeitenYin Yang PrimerAnonymousFarmer100% (6)
- Carbon Dioxide and PH of WaterDokument3 SeitenCarbon Dioxide and PH of Watersilverfox15Noch keine Bewertungen
- CH 9 Animal Transport 2023Dokument46 SeitenCH 9 Animal Transport 2023Mohamed AlyNoch keine Bewertungen
- General Surgery MCQDokument249 SeitenGeneral Surgery MCQShriyansh Chahar88% (8)
- Pleading The Blood Is A Legal Thing!Dokument4 SeitenPleading The Blood Is A Legal Thing!Victor Ramlall100% (1)
- Rahmawati, RENATA FixDokument9 SeitenRahmawati, RENATA Fixannisa fadilasariNoch keine Bewertungen
- Chen Style Tai Chi Cultivating Internal Energy MethodDokument11 SeitenChen Style Tai Chi Cultivating Internal Energy Methodjns198Noch keine Bewertungen
- Normal Laboratory ValuesDokument3 SeitenNormal Laboratory ValuesKMNoch keine Bewertungen
- Mutia Sukma Dewi 2010.04.0.0142 (Jurnal) PDFDokument12 SeitenMutia Sukma Dewi 2010.04.0.0142 (Jurnal) PDFmutiaNoch keine Bewertungen