Das könnte Ihnen auch gefallen
- Life Style Wellness Coaching PDFDokument275 SeitenLife Style Wellness Coaching PDFSundar Prabhu71% (7)
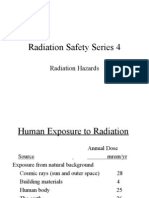
- Radiation Saftey Series 4Dokument26 SeitenRadiation Saftey Series 4johntoblerNoch keine Bewertungen
- Radiation Safety Series 2Dokument31 SeitenRadiation Safety Series 2johntoblerNoch keine Bewertungen
- Radiation Safety Officers Handbook A PDFDokument100 SeitenRadiation Safety Officers Handbook A PDFAlejandro Zubiate100% (1)
- Radiation Protection & Quality Assurance in CT 2018Dokument51 SeitenRadiation Protection & Quality Assurance in CT 2018abafzNoch keine Bewertungen
- Sample Questions For HAAD Prometric and DHA For NursesDokument46 SeitenSample Questions For HAAD Prometric and DHA For NursesJaezelle Ella Sabale100% (4)
- Sample Problems BDokument8 SeitenSample Problems Bapi-308717184Noch keine Bewertungen
- Diagnostic Reference Level in Lumbar Radiography in Abidjan, Côte D'ivoireDokument5 SeitenDiagnostic Reference Level in Lumbar Radiography in Abidjan, Côte D'ivoiretheijesNoch keine Bewertungen
- Healthy FoodDokument13 SeitenHealthy FoodKayden0% (1)
- 2.37 Rso Training Standard Syllabi For Training Courses On Radiological SafetyDokument96 Seiten2.37 Rso Training Standard Syllabi For Training Courses On Radiological SafetyashwiniNoch keine Bewertungen
- Universal Safety (Health) PrecautionsDokument61 SeitenUniversal Safety (Health) Precautionstummalapalli venkateswara rao100% (2)
- Powerpoint DoseDokument16 SeitenPowerpoint DoselcsmfoxNoch keine Bewertungen
- Basic Radiation Safety Awarness TrainingDokument46 SeitenBasic Radiation Safety Awarness TrainingAnton PrasadNoch keine Bewertungen
- Radiation ProtectionDokument50 SeitenRadiation ProtectionDragan GigiNoch keine Bewertungen
- Mock Oral CasesDokument6 SeitenMock Oral Casestcbarot100% (1)
- RadioactivityDokument17 SeitenRadioactivityNurasfiqah AKNoch keine Bewertungen
- Radiation Safety Series 5Dokument10 SeitenRadiation Safety Series 5johntoblerNoch keine Bewertungen
- Radiation Monitoring Procedures in Hospital EnvironmentDokument5 SeitenRadiation Monitoring Procedures in Hospital Environmentnikkitha parker100% (1)
- Radiation Safety Short NotesDokument10 SeitenRadiation Safety Short Notesian3yeung-2Noch keine Bewertungen
- Interaction of Radiation With MatterDokument16 SeitenInteraction of Radiation With MatterRachit KanchanNoch keine Bewertungen
- Chapter 5 Test Radiation Around UsDokument3 SeitenChapter 5 Test Radiation Around UsRaymond Bill Bela-o PatacsilNoch keine Bewertungen
- Refresher & New User Training - 2005Dokument61 SeitenRefresher & New User Training - 2005Abdullah Ahd. AbdulrazigNoch keine Bewertungen
- Lange Q&A: Radiography ExaminationDokument18 SeitenLange Q&A: Radiography ExaminationSamuel JeebanNoch keine Bewertungen
- RSD 4Dokument12 SeitenRSD 4GopakumarNoch keine Bewertungen
- Radiation Dose Limits: Appendix BDokument6 SeitenRadiation Dose Limits: Appendix BVaradha RajanNoch keine Bewertungen
- Radiation Awareness Presentaion (Compatibility Mode)Dokument40 SeitenRadiation Awareness Presentaion (Compatibility Mode)AhmedAmer1100% (1)
- Radiation Quantities & UnitsDokument31 SeitenRadiation Quantities & Unitsdeshpanderavi31100% (2)
- Pe9 Week3 Pe9pf Le H 41Dokument17 SeitenPe9 Week3 Pe9pf Le H 41Edeli Faith PatrocinioNoch keine Bewertungen
- Radiation Safety For General Public WordDokument5 SeitenRadiation Safety For General Public Wordapi-527782385Noch keine Bewertungen
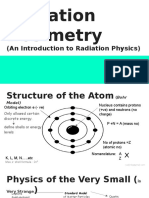
- Radiation Dosimetry (An Introduction To Radiation Physics)Dokument18 SeitenRadiation Dosimetry (An Introduction To Radiation Physics)Linda100% (1)
- Family DeclarationDokument5 SeitenFamily DeclarationVanlal MuanpuiaNoch keine Bewertungen
- Radiation Safety Officer: APS-289-TEDokument5 SeitenRadiation Safety Officer: APS-289-TEfaseeh005100% (1)
- 4 Background RadiationDokument1 Seite4 Background Radiationsomu1100% (1)
- Rad SafetyDokument5 SeitenRad Safetyapi-336647605Noch keine Bewertungen
- C. Attracting An Electron From An Atom.: Dr. Nasser Shubayr Is Massively Proud of You AllDokument33 SeitenC. Attracting An Electron From An Atom.: Dr. Nasser Shubayr Is Massively Proud of You AllghffityNoch keine Bewertungen
- Chapter 16 Radiation Protection and Safety PDFDokument236 SeitenChapter 16 Radiation Protection and Safety PDFAshutosh SinghNoch keine Bewertungen
- The Radiation Chemistry of MacromoleculesVon EverandThe Radiation Chemistry of MacromoleculesMalcolm DoleNoch keine Bewertungen
- Computed Tomography Radiation Safety Issues in OntarioDokument71 SeitenComputed Tomography Radiation Safety Issues in Ontariopebbles18950% (2)
- An Rso Manual Revision July16 2015Dokument363 SeitenAn Rso Manual Revision July16 2015Nevada Technical AssociatesNoch keine Bewertungen
- Science: Quarter 1, WK 2 - Module 2Dokument29 SeitenScience: Quarter 1, WK 2 - Module 2Raniey Mayol100% (1)
- MRSADokument44 SeitenMRSAMarion PerniaNoch keine Bewertungen
- 4 PDFDokument90 Seiten4 PDFGopakumarNoch keine Bewertungen
- Radiographers - Radiation DosimetryDokument33 SeitenRadiographers - Radiation DosimetryAnonymous rYZyQQot55Noch keine Bewertungen
- Radiation Detectors RT70Dokument38 SeitenRadiation Detectors RT70Vitthal DeokateNoch keine Bewertungen
- Shielding Calculations For Radiotherapy Calculation ExamplesDokument6 SeitenShielding Calculations For Radiotherapy Calculation ExamplesJuan DiazNoch keine Bewertungen
- Application For The Post of Senior Medical Physicist / RSO: A.Mohamed MusthafaDokument6 SeitenApplication For The Post of Senior Medical Physicist / RSO: A.Mohamed MusthafaSrujana MNoch keine Bewertungen
- Basic Dosimetric PrincipleDokument73 SeitenBasic Dosimetric Principleradiologi rsud solokNoch keine Bewertungen
- RSO (Medical) Exam SyllabusDokument4 SeitenRSO (Medical) Exam SyllabusSargunan SabNoch keine Bewertungen
- Lecture Notes Finals RT 208Dokument5 SeitenLecture Notes Finals RT 208Giralph NikkoNoch keine Bewertungen
- Part 2 Week 9 - Treatment PlanningDokument50 SeitenPart 2 Week 9 - Treatment PlanningdanNoch keine Bewertungen
- Discovery of RadiationDokument13 SeitenDiscovery of RadiationAdel SukerNoch keine Bewertungen
- 2 Fundamental Principles of RadiobiologyDokument28 Seiten2 Fundamental Principles of RadiobiologyAngelo RamosNoch keine Bewertungen
- ICRP 53 - Radiation Dose To Patients From RadiopharmaceuticalsDokument340 SeitenICRP 53 - Radiation Dose To Patients From Radiopharmaceuticalsraymond_lane_7Noch keine Bewertungen
- Radiation DosimetryDokument18 SeitenRadiation DosimetrySmita SharmaNoch keine Bewertungen
- Radioacitvity PDFDokument14 SeitenRadioacitvity PDFArjun RavalNoch keine Bewertungen
- Aapm Report No. 16 Protocol For HeavyDokument60 SeitenAapm Report No. 16 Protocol For HeavyLaurentiu RadoiNoch keine Bewertungen
- Extra Credit Problems Submit Upto 20 QuesDokument7 SeitenExtra Credit Problems Submit Upto 20 Quesapi-174496267Noch keine Bewertungen
- RadiationDokument30 SeitenRadiationGadis PodehNoch keine Bewertungen
- 1 C Intro To Nuclear ChemistryDokument41 Seiten1 C Intro To Nuclear ChemistryNur Intan JunaediNoch keine Bewertungen
- Radiation Protection (Module 1.1)Dokument32 SeitenRadiation Protection (Module 1.1)ado666eddieNoch keine Bewertungen
- Radiation Biology QuestionsDokument2 SeitenRadiation Biology QuestionsRoxy Marie ChanNoch keine Bewertungen
- Compton Academy 2023Dokument8 SeitenCompton Academy 2023Sargunan SabNoch keine Bewertungen
- Sources, Fields, Measurements, and Applications: Radiation Dosimetry, Vol. 3Von EverandSources, Fields, Measurements, and Applications: Radiation Dosimetry, Vol. 3Frank H. AttixNoch keine Bewertungen
- Advances in Biological and Medical Physics: Volume 1Von EverandAdvances in Biological and Medical Physics: Volume 1Noch keine Bewertungen
- 01 - Radiation Protection 1 - WM 2013Dokument42 Seiten01 - Radiation Protection 1 - WM 2013Amr MuhammedNoch keine Bewertungen
- D OSE S and S Ources of Rad I AT I ON ExposureDokument47 SeitenD OSE S and S Ources of Rad I AT I ON ExposureAinah CredoNoch keine Bewertungen
- Dr. Rita Zahara, SP - OkDokument68 SeitenDr. Rita Zahara, SP - OkRamadani NazarNoch keine Bewertungen
- Radiation Protection in Diagnostic and Interventional RadiologyDokument44 SeitenRadiation Protection in Diagnostic and Interventional RadiologyPaul KennedyNoch keine Bewertungen
- Radiation Quantities and Units - Joe Berresford - 13th MayDokument41 SeitenRadiation Quantities and Units - Joe Berresford - 13th MayAmr MuhammedNoch keine Bewertungen
- Principles of Radiation OncologyDokument22 SeitenPrinciples of Radiation OncologyGina RNoch keine Bewertungen
- Automation in PlanningDokument38 SeitenAutomation in PlanningGina RNoch keine Bewertungen
- Brachytherapy 2Dokument59 SeitenBrachytherapy 2Gina R0% (1)
- PTW PresentationDokument44 SeitenPTW PresentationGina RNoch keine Bewertungen
- Fundamental Radiobiology 2019Dokument54 SeitenFundamental Radiobiology 2019Gina R100% (1)
- Medical Physics Present and FutureDokument59 SeitenMedical Physics Present and FutureGina RNoch keine Bewertungen
- Tolerance and Adverse Event Profile With SorafenibDokument3 SeitenTolerance and Adverse Event Profile With SorafenibGina RNoch keine Bewertungen
- Very Low Doses of Ionizing Radiation and Redox Associated Modifiers, Free Radical Biology & Medicine 99 (2016) 110-119Dokument10 SeitenVery Low Doses of Ionizing Radiation and Redox Associated Modifiers, Free Radical Biology & Medicine 99 (2016) 110-119Gina RNoch keine Bewertungen
- Hili MallDokument7 SeitenHili Mallvenkatesh snkNoch keine Bewertungen
- Msds - AdditiveDokument9 SeitenMsds - AdditivedanalabNoch keine Bewertungen
- Work Life Balance WLB QuestionnaireDokument3 SeitenWork Life Balance WLB QuestionnairetarisaiNoch keine Bewertungen
- Guidelines For Handling Medico Legal CasesDokument5 SeitenGuidelines For Handling Medico Legal CasesVaishnavi Jayakumar80% (5)
- Acute Pancriatis Special HDokument9 SeitenAcute Pancriatis Special HInga CeagleiNoch keine Bewertungen
- Module 7 Lesson 4Dokument31 SeitenModule 7 Lesson 4MA EDYLYN NOGUERRANoch keine Bewertungen
- Nepheline Syenite - Various Grades (A200-A270)Dokument5 SeitenNepheline Syenite - Various Grades (A200-A270)Lynne MarrNoch keine Bewertungen
- PR 1 ResearchDokument22 SeitenPR 1 ResearchLawrence LuceñoNoch keine Bewertungen
- MMHA - Decriminalization & Thresholds - CPT Members - April 21, 2022Dokument6 SeitenMMHA - Decriminalization & Thresholds - CPT Members - April 21, 2022Tyler HarperNoch keine Bewertungen
- PBL Planning PDFDokument3 SeitenPBL Planning PDFLai Chee ShengNoch keine Bewertungen
- Trypsin ChymotrypsinDokument6 SeitenTrypsin ChymotrypsinKalpana Shubhangi BhedaNoch keine Bewertungen
- HorlicksDokument5 SeitenHorlicksAdalberto MacdonaldNoch keine Bewertungen
- DKD DR RatnaDokument29 SeitenDKD DR Ratnaxiongmao2389Noch keine Bewertungen
- Gynae Training ManualDokument30 SeitenGynae Training ManualKhushi Husna100% (1)
- Cossh Risk Assessment: Carried Out By: Department: Date: Substance Name: CRA NumberDokument2 SeitenCossh Risk Assessment: Carried Out By: Department: Date: Substance Name: CRA NumberNiraNoch keine Bewertungen
- Features of CHN: Learning ObjectivesDokument6 SeitenFeatures of CHN: Learning ObjectivesAkeroNoch keine Bewertungen
- Micro Labs - STF Division Products...Dokument17 SeitenMicro Labs - STF Division Products...micro sobanNoch keine Bewertungen
- Renfrew County Community Study Executive SummaryDokument24 SeitenRenfrew County Community Study Executive SummaryShawna BabcockNoch keine Bewertungen
- Technology Process Fortification Ruchika SachdevaDokument23 SeitenTechnology Process Fortification Ruchika SachdevaHimex EquipmentsNoch keine Bewertungen
- DM Infectious DiseasesDokument20 SeitenDM Infectious DiseasesVasishta NadellaNoch keine Bewertungen
- MScHandbook Imperial Chemical EnggDokument87 SeitenMScHandbook Imperial Chemical EnggMurugeshNoch keine Bewertungen