Das könnte Ihnen auch gefallen
- Thesis Systemic Lupus ErythematosusDokument6 SeitenThesis Systemic Lupus Erythematosuscaitlinwilsonsavannah100% (2)
- Systemic Lupus Erythematosus Research PapersDokument6 SeitenSystemic Lupus Erythematosus Research Papersebvjkbaod100% (3)
- SLE Pathogenesis, Diagnosis and Tailoring TherapyDokument66 SeitenSLE Pathogenesis, Diagnosis and Tailoring TherapyWenny TanyawanNoch keine Bewertungen
- Approach To Lymphadenopathy: February 15, 2017Dokument9 SeitenApproach To Lymphadenopathy: February 15, 2017LativaSusantiNoch keine Bewertungen
- SLE Care: Systemic Lupus Erythematosus Signs, Symptoms, and Nursing ResponsibilitiesDokument8 SeitenSLE Care: Systemic Lupus Erythematosus Signs, Symptoms, and Nursing ResponsibilitiesampalNoch keine Bewertungen
- Int14 SLEDokument17 SeitenInt14 SLEOsama AlhumisiNoch keine Bewertungen
- Outline For Lupus Research PaperDokument5 SeitenOutline For Lupus Research Paperegx2asvt100% (1)
- Term Paper On LupusDokument7 SeitenTerm Paper On Lupusc5qvf1q1100% (1)
- Presentation by Muhammad Asyraf Bin Hj. Ariffin: Diploma in Pharmacy PH 110 Anatomy & Physiology PHC 121Dokument21 SeitenPresentation by Muhammad Asyraf Bin Hj. Ariffin: Diploma in Pharmacy PH 110 Anatomy & Physiology PHC 121Muhammad AsyrafNoch keine Bewertungen
- Systemic Lupus Erythematosus - Immunity PDFDokument7 SeitenSystemic Lupus Erythematosus - Immunity PDFTõkå MøhámmêdNoch keine Bewertungen
- Systemiclupus Erythematosus: Safeandeffective Managementin PrimarycareDokument12 SeitenSystemiclupus Erythematosus: Safeandeffective Managementin PrimarycareWilda Dwi FijriyantiNoch keine Bewertungen
- 9 16 1 SM PDFDokument5 Seiten9 16 1 SM PDFjeka222Noch keine Bewertungen
- 15 SleDokument41 Seiten15 Sleزياد سعيدNoch keine Bewertungen
- Diagnosing and Managing Systemic Lupus ErythematosusDokument3 SeitenDiagnosing and Managing Systemic Lupus ErythematosusAlya Putri KhairaniNoch keine Bewertungen
- Sle SlidesDokument42 SeitenSle SlidesAzizan HannyNoch keine Bewertungen
- Research Paper On LupusDokument4 SeitenResearch Paper On Lupusfyrj7h9z100% (1)
- Lupus Research Paper ThesisDokument7 SeitenLupus Research Paper Thesisgz8reqdc100% (1)
- Research Paper Multiple SclerosisDokument5 SeitenResearch Paper Multiple Sclerosisafednfsfq100% (1)
- Systemic Lupus Erythematosus (SLE) Pathogenesis and Diagnostic CriteriaDokument96 SeitenSystemic Lupus Erythematosus (SLE) Pathogenesis and Diagnostic CriteriaDon CaprettoNoch keine Bewertungen
- Dry Eye Atau Mata KerigDokument53 SeitenDry Eye Atau Mata Kerigpemburu_gratisNoch keine Bewertungen
- Topic 8 Differential Diagnosis of FUO SCTD - Short.Dokument76 SeitenTopic 8 Differential Diagnosis of FUO SCTD - Short.hhbhhNoch keine Bewertungen
- Nihms 362971 PDFDokument24 SeitenNihms 362971 PDFiliepopNoch keine Bewertungen
- Diffuse Large-B-Cell Lymphoma Caso PDFDokument7 SeitenDiffuse Large-B-Cell Lymphoma Caso PDFAlejandra BarlettaNoch keine Bewertungen
- Lupus Research Paper OutlineDokument5 SeitenLupus Research Paper Outlinezwyzywzjf100% (1)
- Multiple Sclerosis Thesis PDFDokument6 SeitenMultiple Sclerosis Thesis PDFKarla Long100% (2)
- Multiple Sclerosis Research Paper OutlineDokument6 SeitenMultiple Sclerosis Research Paper Outlinevbbcvwplg100% (1)
- Care of Unconscious PatientDokument6 SeitenCare of Unconscious PatientSuparna SinghaNoch keine Bewertungen
- Group 3 - SLEDokument10 SeitenGroup 3 - SLEronhadjess14Noch keine Bewertungen
- Epilepsy Research Paper ConclusionDokument7 SeitenEpilepsy Research Paper Conclusionzpyrufrif100% (1)
- Vasculitis in ChildrenDokument22 SeitenVasculitis in ChildrenRashed ShatnawiNoch keine Bewertungen
- Lupus ErythematosusDokument5 SeitenLupus ErythematosusAkshay SatputeNoch keine Bewertungen
- RA & SLE Kuliah Blok 2014 EditDokument75 SeitenRA & SLE Kuliah Blok 2014 EditAdi ParamarthaNoch keine Bewertungen
- Pediatric Demyelinating Diseases of The Central Nervous System and Their MimicsDokument338 SeitenPediatric Demyelinating Diseases of The Central Nervous System and Their MimicsVu Hoang100% (1)
- Clinical Review: Systemic Lupus ErythematosusDokument5 SeitenClinical Review: Systemic Lupus ErythematosusVijeyachandhar DorairajNoch keine Bewertungen
- Epilepsy Research Paper PDFDokument8 SeitenEpilepsy Research Paper PDFyscgudvnd100% (1)
- SLE MedscapeDokument49 SeitenSLE MedscapeAndino FadilNoch keine Bewertungen
- Jurnal Reading Rehab Medik + TranslateDokument16 SeitenJurnal Reading Rehab Medik + TranslatekristiviaNoch keine Bewertungen
- Research Paper Alzheimer DiseaseDokument5 SeitenResearch Paper Alzheimer Diseasefzjzn694100% (1)
- Case Discussion SLEDokument4 SeitenCase Discussion SLERanjeetha SivaNoch keine Bewertungen
- Neonatal Lupus Erythematosus: Extracutaneous Findings and Diagnostic WorkupDokument2 SeitenNeonatal Lupus Erythematosus: Extracutaneous Findings and Diagnostic WorkupNatasha AmaldaNoch keine Bewertungen
- Thesis Statement Examples Alzheimers DiseaseDokument6 SeitenThesis Statement Examples Alzheimers DiseaseJulie Davis100% (2)
- Case Study For Multiple SclerosisDokument4 SeitenCase Study For Multiple SclerosisGabbii CincoNoch keine Bewertungen
- About Scleroderma: Frequently Asked QuestionsDokument2 SeitenAbout Scleroderma: Frequently Asked QuestionsArja' WaasNoch keine Bewertungen
- FS007v1 RasmussensDokument4 SeitenFS007v1 Rasmussensbilly2107Noch keine Bewertungen
- LupusDokument9 SeitenLupusyresendiz93Noch keine Bewertungen
- Rheumatoid ArthritisDokument4 SeitenRheumatoid ArthritisShinta ArumadinaNoch keine Bewertungen
- CIDPDokument21 SeitenCIDPidno1008Noch keine Bewertungen
- Levy 2012Dokument20 SeitenLevy 2012Anonymous ujOv31SNoch keine Bewertungen
- Lupus Research PaperDokument5 SeitenLupus Research Paperttdqgsbnd100% (3)
- New York State Department of Health Systemic Lupus ErythematosusDokument3 SeitenNew York State Department of Health Systemic Lupus ErythematosusCaryl Joy Dela PeñaNoch keine Bewertungen
- College Research Paper On LupusDokument7 SeitenCollege Research Paper On Lupusafnkedekzbezsb100% (1)
- Lupus ErythematosusDokument5 SeitenLupus ErythematosusAditya DarmawanNoch keine Bewertungen
- Mitsumoto ALS JAMA07Dokument11 SeitenMitsumoto ALS JAMA07abcdefgNoch keine Bewertungen
- Research Papers Alzheimers DiseaseDokument7 SeitenResearch Papers Alzheimers Diseaseegja0g11100% (1)
- Mixed Connective Tissue DZ (SLE + Scleroderma)Dokument7 SeitenMixed Connective Tissue DZ (SLE + Scleroderma)AshbirZammeriNoch keine Bewertungen
- Lupus 101Dokument10 SeitenLupus 101melodia gandezaNoch keine Bewertungen
- Part 1Dokument58 SeitenPart 1Abdulrahman KatibNoch keine Bewertungen
- Dandy-Walker Syndrome Patients - GREEN AAMDokument35 SeitenDandy-Walker Syndrome Patients - GREEN AAMdonilord19Noch keine Bewertungen
- Community Health Nursing Practice QuestionsDokument17 SeitenCommunity Health Nursing Practice QuestionsJho MagadanNoch keine Bewertungen
- AmebaDokument21 SeitenAmebamihaelaemma100% (2)
- The Ultimate Guide To KetoDokument48 SeitenThe Ultimate Guide To KetoleosantillanNoch keine Bewertungen
- The Abington Journal 07-04-2012Dokument22 SeitenThe Abington Journal 07-04-2012The Times LeaderNoch keine Bewertungen
- Lung Cancer Presentation: DR Richard Sullivan and Ms Anne FraserDokument24 SeitenLung Cancer Presentation: DR Richard Sullivan and Ms Anne FraseranggiNoch keine Bewertungen
- Silibin PhosphatidylcholineDokument6 SeitenSilibin PhosphatidylcholineJayen BarochiaNoch keine Bewertungen
- Internal Medicine - DermatologyDokument125 SeitenInternal Medicine - DermatologySoleil DaddouNoch keine Bewertungen
- Health Statement FormDokument2 SeitenHealth Statement FormRose Ann DuqueNoch keine Bewertungen
- DOHNS Part II OSCE Glasgow May 2013Dokument4 SeitenDOHNS Part II OSCE Glasgow May 2013rizwan afzal100% (2)
- Skin DisordersDokument4 SeitenSkin DisordersAj PotXzs Ü100% (2)
- What Is Cancer? What Causes Cancer?: Discovered An Important Clue As To Why Cancer Cells SpreadDokument8 SeitenWhat Is Cancer? What Causes Cancer?: Discovered An Important Clue As To Why Cancer Cells SpreadAlfred Melvin SolivaNoch keine Bewertungen
- CC CCCCC: Y CCC CCCC CCCCC CCCC CCC CCCCCCCCCC CC CDokument3 SeitenCC CCCCC: Y CCC CCCC CCCCC CCCC CCC CCCCCCCCCC CC CRachel Ann BatayolaNoch keine Bewertungen
- Study of Drug Delivery Through Metallic Nanoparticles in Therapeutics of Ocular MelanomaDokument14 SeitenStudy of Drug Delivery Through Metallic Nanoparticles in Therapeutics of Ocular MelanomaSara IrshadNoch keine Bewertungen
- 5 Minute Fluency - Volume IDokument79 Seiten5 Minute Fluency - Volume IAlexandre Magno AlvesNoch keine Bewertungen
- ToacsDokument3 SeitenToacsdr_shafiqNoch keine Bewertungen
- Large Intestine HistologyDokument24 SeitenLarge Intestine HistologyMudassar RoomiNoch keine Bewertungen
- Glands and HormonesDokument1 SeiteGlands and HormonesRussel Dave ValenzuelaNoch keine Bewertungen
- Aplastic Anemia and HomoeopathyDokument3 SeitenAplastic Anemia and HomoeopathyDr. Rajneesh Kumar Sharma MD Hom100% (1)
- Material Safety Data Sheet: 1. Product and Company IdentificationDokument9 SeitenMaterial Safety Data Sheet: 1. Product and Company IdentificationAdeNoch keine Bewertungen
- Pemeriksaan Fisik ThoraxDokument16 SeitenPemeriksaan Fisik ThoraxYudiWatanabeNoch keine Bewertungen
- IMRT - ACR - ASTRO GuidelinesDokument11 SeitenIMRT - ACR - ASTRO GuidelinesSayan DasNoch keine Bewertungen
- ACETIC ACID REMEDIESDokument55 SeitenACETIC ACID REMEDIESEngr Syed Numan ShahNoch keine Bewertungen
- Dr. Reckeweg R59 Drops for Obesity TreatmentDokument6 SeitenDr. Reckeweg R59 Drops for Obesity TreatmentSiddharth MedicareNoch keine Bewertungen
- Revlon Case StudyDokument5 SeitenRevlon Case StudyAriel Anthonie Puso GarciaNoch keine Bewertungen
- Jake's PrognosisDokument3 SeitenJake's PrognosisSiegNoch keine Bewertungen
- Human PhysiologyDokument125 SeitenHuman PhysiologyVitalis MbuyaNoch keine Bewertungen
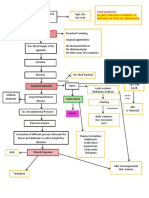
- CPC - Appendicitis (Flowchart)Dokument1 SeiteCPC - Appendicitis (Flowchart)Milet NacionalesNoch keine Bewertungen
- A Theory-Based Decision Aid FoDokument12 SeitenA Theory-Based Decision Aid FoAnonymous vUl83IptiSNoch keine Bewertungen
- From First Symptoms To Diagnosis: Initial Clinical Presentation of Primary Brain TumorsDokument7 SeitenFrom First Symptoms To Diagnosis: Initial Clinical Presentation of Primary Brain TumorsMohammad AamirNoch keine Bewertungen