Das könnte Ihnen auch gefallen
- Disseminated Intravascular CoagualationDokument47 SeitenDisseminated Intravascular CoagualationIshaBrijeshSharmaNoch keine Bewertungen
- Systemic SclerosisDokument36 SeitenSystemic SclerosisrgardónNoch keine Bewertungen
- Surviving Leukemia and Hodgkin's Lymphoma: An Overview Of Effective Treatment MethodsVon EverandSurviving Leukemia and Hodgkin's Lymphoma: An Overview Of Effective Treatment MethodsNoch keine Bewertungen
- Jurnal ReadingDokument21 SeitenJurnal ReadingWb Iqbal Tendi AlamNoch keine Bewertungen
- Department of Internal Medicine Iii Hemorrhagic Syndromes: - Rajkumar Subasaravanan Subgroup "12"Dokument122 SeitenDepartment of Internal Medicine Iii Hemorrhagic Syndromes: - Rajkumar Subasaravanan Subgroup "12"Suba Saravanan 12Noch keine Bewertungen
- Fast Facts: Familial Chylomicronemia Syndrome: Raising awareness of a rare genetic diseaseVon EverandFast Facts: Familial Chylomicronemia Syndrome: Raising awareness of a rare genetic diseaseNoch keine Bewertungen
- AssignmentDokument11 SeitenAssignmentrehamoh1997Noch keine Bewertungen
- Glomerular DsDokument18 SeitenGlomerular Dsnathan asfahaNoch keine Bewertungen
- Systemic Sclerosis (SSCL)Dokument4 SeitenSystemic Sclerosis (SSCL)AtoNoch keine Bewertungen
- Giant Cell Arteritis, A Simple Guide To The Condition, Treatment And Related DiseasesVon EverandGiant Cell Arteritis, A Simple Guide To The Condition, Treatment And Related DiseasesNoch keine Bewertungen
- Nbme 11 ExplainationDokument55 SeitenNbme 11 Explainationazankhan9960% (10)
- Leg UlcersDokument14 SeitenLeg UlcersNovi Y'uZzmanNoch keine Bewertungen
- Deep Vein Thrombosis and Pulmonary Embolism: A guide for practitioners 2/edVon EverandDeep Vein Thrombosis and Pulmonary Embolism: A guide for practitioners 2/edBewertung: 5 von 5 Sternen5/5 (1)
- Inflammatory Bowel Disease: Dr. J V Srujan MDDokument42 SeitenInflammatory Bowel Disease: Dr. J V Srujan MDharika hariNoch keine Bewertungen
- Systemic Sclerosis (Scleroderma)Dokument3 SeitenSystemic Sclerosis (Scleroderma)AtiqahNoch keine Bewertungen
- CK SamplesDokument63 SeitenCK SamplesAppu ayyala100% (2)
- Hematology Mccq1Dokument236 SeitenHematology Mccq1javaheri.abdorrazaghNoch keine Bewertungen
- Nbme 11Dokument102 SeitenNbme 11Mohamed Nabil100% (36)
- Hemostatic Complications of Solid OrganDokument18 SeitenHemostatic Complications of Solid OrganWael AlkhiaryNoch keine Bewertungen
- Hematologic Disorders Causing Massive Splenomegaly and AnemiaDokument9 SeitenHematologic Disorders Causing Massive Splenomegaly and AnemiaMathew S PeedikayilNoch keine Bewertungen
- The Spleen: Schwartz's Principles of Surgery 11th EdDokument54 SeitenThe Spleen: Schwartz's Principles of Surgery 11th EdaddelinsNoch keine Bewertungen
- Vasculitis SyndromesDokument13 SeitenVasculitis Syndromesnitinmaripeddi7Noch keine Bewertungen
- Derma GITDokument48 SeitenDerma GITapi-3843372Noch keine Bewertungen
- Nephrotic SyndromeDokument12 SeitenNephrotic SyndromePutra Fatkhul Rizqi QoroidNoch keine Bewertungen
- Bone Marrow Failure 2008-09Dokument15 SeitenBone Marrow Failure 2008-09Karan BhattNoch keine Bewertungen
- Set 3 COMP-2Dokument71 SeitenSet 3 COMP-2Appu ayyalaNoch keine Bewertungen
- The Spleen: Schwartz's Principles of Surgery 11th EdDokument54 SeitenThe Spleen: Schwartz's Principles of Surgery 11th EdMuhammad Fhandeka IsrarNoch keine Bewertungen
- Michael W, COMAT SurgeryDokument14 SeitenMichael W, COMAT SurgerySeanNoch keine Bewertungen
- Literature AbdoDokument20 SeitenLiterature AbdothestaffforpediatricptNoch keine Bewertungen
- SplenomegalyDokument4 SeitenSplenomegalydoctorimrankabirNoch keine Bewertungen
- HepatosplenomegalyDokument52 SeitenHepatosplenomegalySundar NatarajanNoch keine Bewertungen
- Disseminated Intravascular Coagulation (DIC) : PhysicalDokument4 SeitenDisseminated Intravascular Coagulation (DIC) : PhysicalHadi AbdullahNoch keine Bewertungen
- Henoch - Schonlein Purpura (HSP) : - It Is The Most Common Cause of Non-Thrombocytopenic Purpura in ChildrenDokument23 SeitenHenoch - Schonlein Purpura (HSP) : - It Is The Most Common Cause of Non-Thrombocytopenic Purpura in ChildrenLaith DmourNoch keine Bewertungen
- Nephrotic SyndromeDokument5 SeitenNephrotic SyndromeAnjhiene CambaNoch keine Bewertungen
- Disorder of PlateletsDokument27 SeitenDisorder of PlateletsRoby KieranNoch keine Bewertungen
- Skin Problems in Chronic KidneyDokument73 SeitenSkin Problems in Chronic KidneyMunir MughalNoch keine Bewertungen
- Quick Review/Pearl Sheet: These Are in Random Order To Help You Prepare For You NBME ExamDokument19 SeitenQuick Review/Pearl Sheet: These Are in Random Order To Help You Prepare For You NBME ExamWyoXPat100% (11)
- 2 Glomerular DiseasesDokument48 Seiten2 Glomerular DiseasesDammaqsaa W BiyyanaaNoch keine Bewertungen
- SNDokument7 SeitenSNArdy Syahabuddin GofarNoch keine Bewertungen
- Renal and Urinary System PathologyDokument70 SeitenRenal and Urinary System PathologykiflomNoch keine Bewertungen
- BLEEDING DISORDERS - FinalDokument41 SeitenBLEEDING DISORDERS - Finalsteph.apondiNoch keine Bewertungen
- Ojim 2016091213324550Dokument10 SeitenOjim 2016091213324550rianmg21Noch keine Bewertungen
- VasculitisDokument184 SeitenVasculitisRada NemirovskiNoch keine Bewertungen
- MRCPCH Guide Heme: A Hypochromic MicrocyticDokument8 SeitenMRCPCH Guide Heme: A Hypochromic MicrocyticRajiv KabadNoch keine Bewertungen
- Vasculitis 1Dokument47 SeitenVasculitis 1Rusty RyanNoch keine Bewertungen
- Rheumatoid Arthritis and Acute Rheumatic FeverDokument76 SeitenRheumatoid Arthritis and Acute Rheumatic FeverM. O. PHC HOLAVANAHALLYNoch keine Bewertungen
- Angio EdemaDokument9 SeitenAngio EdemaJavierNoch keine Bewertungen
- Disorders of The Lymphatic System: AnatomyDokument3 SeitenDisorders of The Lymphatic System: AnatomyyusufNoch keine Bewertungen
- Photo QuizDokument21 SeitenPhoto Quizabas_maytham1021100% (3)
- 4 - VasculitisDokument22 Seiten4 - VasculitisIrakli GhlontiNoch keine Bewertungen
- Nephrotic Syndrome in Adults: Acute Medicine 2018 17 (1) : 36-43 36Dokument8 SeitenNephrotic Syndrome in Adults: Acute Medicine 2018 17 (1) : 36-43 36Deddy TriwijayaNoch keine Bewertungen
- Lymphedema 101: Part 1: Understanding The Pathology and DiagnosisDokument5 SeitenLymphedema 101: Part 1: Understanding The Pathology and DiagnosisSAKAI69Noch keine Bewertungen
- All About Pleural EffusionDokument6 SeitenAll About Pleural EffusionTantin KristantoNoch keine Bewertungen
- AmyloidosisDokument2 SeitenAmyloidosisLanaAmerieNoch keine Bewertungen
- WK4: Menopause and Sexual Dysfx: - First Change in Menopause Is Decreased InhibinDokument2 SeitenWK4: Menopause and Sexual Dysfx: - First Change in Menopause Is Decreased InhibinLanaAmerieNoch keine Bewertungen
- Ah PDFDokument134 SeitenAh PDFLanaAmerieNoch keine Bewertungen
- Depression TretDokument1 SeiteDepression TretLanaAmerieNoch keine Bewertungen
- SLE SketchyDokument2 SeitenSLE SketchyLanaAmerieNoch keine Bewertungen
- Table 1: Infective Endocarditis Non Infective Myocarditis Myocardidits PericarditisDokument3 SeitenTable 1: Infective Endocarditis Non Infective Myocarditis Myocardidits PericarditisLanaAmerieNoch keine Bewertungen
- WelcomeDokument5 SeitenWelcomeCatNoch keine Bewertungen
- Table 1: Infective Endocarditis Non Infective Myocarditis Myocardidits PericarditisDokument3 SeitenTable 1: Infective Endocarditis Non Infective Myocarditis Myocardidits PericarditisLanaAmerieNoch keine Bewertungen
- IN10 PharmyDokument7 SeitenIN10 PharmyLanaAmerieNoch keine Bewertungen
- Congenital Anomalies of Kidney and Lowe Urinary TractDokument2 SeitenCongenital Anomalies of Kidney and Lowe Urinary TractLanaAmerieNoch keine Bewertungen
- Integumentary Lec 1: Overview of The Integument: A-Integumentary (Skin) SystemDokument6 SeitenIntegumentary Lec 1: Overview of The Integument: A-Integumentary (Skin) SystemLanaAmerieNoch keine Bewertungen
- Cluster of Lesions, PapularDokument3 SeitenCluster of Lesions, PapularLanaAmerieNoch keine Bewertungen
- Macules Macules and Papules Papules VesiclesDokument6 SeitenMacules Macules and Papules Papules VesiclesLanaAmerieNoch keine Bewertungen
- IN10 PharmyDokument7 SeitenIN10 PharmyLanaAmerieNoch keine Bewertungen
- OPP - Lab - Counterstrain - Ribs, Anterior, PosteriorDokument1 SeiteOPP - Lab - Counterstrain - Ribs, Anterior, PosteriorLanaAmerieNoch keine Bewertungen
- RNL DruDokument1 SeiteRNL DruLanaAmerieNoch keine Bewertungen
- Skin PDFDokument13 SeitenSkin PDFLanaAmerieNoch keine Bewertungen
- Integumentary Lec 1: Overview of The Integument: A-Integumentary (Skin) SystemDokument6 SeitenIntegumentary Lec 1: Overview of The Integument: A-Integumentary (Skin) SystemLanaAmerieNoch keine Bewertungen
- Urinery IncontinsetenceDokument1 SeiteUrinery IncontinsetenceLanaAmerieNoch keine Bewertungen
- Platelets PDFDokument65 SeitenPlatelets PDFLana AmerieNoch keine Bewertungen
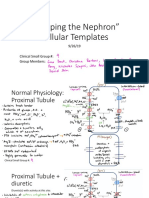
- "Mapping The Nephron" Cellular Templates: Gina Bartoni Lana Daniel ShinDokument11 Seiten"Mapping The Nephron" Cellular Templates: Gina Bartoni Lana Daniel ShinLanaAmerieNoch keine Bewertungen
- OPP - Lab - Counterstrain - Ribs, Anterior, PosteriorDokument1 SeiteOPP - Lab - Counterstrain - Ribs, Anterior, PosteriorLanaAmerieNoch keine Bewertungen
- Biochemistry 7Th Edition Berg Test Bank Full Chapter PDFDokument29 SeitenBiochemistry 7Th Edition Berg Test Bank Full Chapter PDFciaramilcahbrpe100% (11)
- 2 Long Exam Feedback: BiochemistryDokument7 Seiten2 Long Exam Feedback: BiochemistryManila MedNoch keine Bewertungen
- Acquired Platelet Dysfunction With Eosinophilia (APDE)Dokument4 SeitenAcquired Platelet Dysfunction With Eosinophilia (APDE)Rahmat FirdausNoch keine Bewertungen
- The Blood Clotting MechanismDokument20 SeitenThe Blood Clotting Mechanismzynab123Noch keine Bewertungen
- Disorders of The Digestive SystemDokument3 SeitenDisorders of The Digestive SystemɪQ ʟᴇᴠᴇʟ 148ˊˎ-Noch keine Bewertungen
- Transes HemaDokument4 SeitenTranses HemaJainee Chen JavillonarNoch keine Bewertungen
- Stationary Versus Agitated Storage of Whole Blood.6 PDFDokument5 SeitenStationary Versus Agitated Storage of Whole Blood.6 PDFAngel CallesNoch keine Bewertungen
- Farmakologi Obat Hemostasis & AntikoagulanDokument19 SeitenFarmakologi Obat Hemostasis & AntikoagulanamirahNoch keine Bewertungen
- KampoloDokument26 SeitenKampoloSalifyanji SimpambaNoch keine Bewertungen
- CA Series Measurement Evaluation and Check MethodsDokument34 SeitenCA Series Measurement Evaluation and Check MethodsmarianalinamihaelaNoch keine Bewertungen
- Oral Surgery Part - IDokument7 SeitenOral Surgery Part - ISushma Bezwada100% (1)
- Hematological DisordersDokument9 SeitenHematological DisordersFoxtrot NursingNoch keine Bewertungen
- Phlebotomy TestDokument11 SeitenPhlebotomy TestRaquel Girón75% (4)
- Assessment Diagnosis Inference Planning Intervention Rationale EvaluationDokument6 SeitenAssessment Diagnosis Inference Planning Intervention Rationale EvaluationnjmalabananNoch keine Bewertungen
- Newer Oral Anticoagulant: DR Shivaom Chaurasia Resident Internal MedicineDokument57 SeitenNewer Oral Anticoagulant: DR Shivaom Chaurasia Resident Internal MedicineMuhammad Reza FirdausNoch keine Bewertungen
- Human Biology CirculationDokument94 SeitenHuman Biology CirculationJuiced-IN itNoch keine Bewertungen
- En C#k#prest 20180228Dokument1 SeiteEn C#k#prest 20180228dian fantriNoch keine Bewertungen
- Unit 4 Study Guide PathoDokument10 SeitenUnit 4 Study Guide Pathoangieswenson100% (1)
- UM Coag - 4D EN USERDokument48 SeitenUM Coag - 4D EN USERT KNoch keine Bewertungen
- Lipid Lowering Agents IDokument14 SeitenLipid Lowering Agents IRALPH ELVIN MACANLALAYNoch keine Bewertungen
- Pre - and Post-Operative Monitoring of PatientsDokument90 SeitenPre - and Post-Operative Monitoring of Patientssarguss1490% (21)
- Intro To HematologyDokument9 SeitenIntro To HematologyDayledaniel SorvetoNoch keine Bewertungen
- Octaplex File FullDokument369 SeitenOctaplex File FullAhmed100% (1)
- Pharmacology A ReviewDokument13 SeitenPharmacology A ReviewCheriz LukbanNoch keine Bewertungen
- Ap - BloodDokument13 SeitenAp - BloodJustine May Balinggan DelmasNoch keine Bewertungen
- IV Therapy SlidesDokument8 SeitenIV Therapy SlidesRegean MercadoNoch keine Bewertungen
- Transfusi: Ristiawan Muji Laksono Lab/Smf Anestesi Dan Terapi Intensif Fkub-RssaDokument34 SeitenTransfusi: Ristiawan Muji Laksono Lab/Smf Anestesi Dan Terapi Intensif Fkub-RssaBryand KostaNoch keine Bewertungen
- Nicola Maffulli (Eds.) - Platelet Rich Plasma in Musculoskeletal Practice-Springer-Verlag London (2016) PDFDokument256 SeitenNicola Maffulli (Eds.) - Platelet Rich Plasma in Musculoskeletal Practice-Springer-Verlag London (2016) PDFedbraga-1Noch keine Bewertungen
- Essay On PathwaysDokument3 SeitenEssay On PathwaysChristian MahabirNoch keine Bewertungen
- Drop MethodDokument2 SeitenDrop MethodCharlene Bularan100% (2)
- By the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsVon EverandBy the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsNoch keine Bewertungen
- Summary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisVon EverandSummary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisBewertung: 4.5 von 5 Sternen4.5/5 (42)
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeVon EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeBewertung: 2 von 5 Sternen2/5 (1)
- Raising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsVon EverandRaising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsBewertung: 5 von 5 Sternen5/5 (1)
- The Age of Magical Overthinking: Notes on Modern IrrationalityVon EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityBewertung: 4 von 5 Sternen4/5 (24)
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedVon EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedBewertung: 5 von 5 Sternen5/5 (80)
- The Comfort of Crows: A Backyard YearVon EverandThe Comfort of Crows: A Backyard YearBewertung: 4.5 von 5 Sternen4.5/5 (23)
- The Obesity Code: Unlocking the Secrets of Weight LossVon EverandThe Obesity Code: Unlocking the Secrets of Weight LossBewertung: 4 von 5 Sternen4/5 (6)
- The Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaVon EverandThe Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- Raising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsVon EverandRaising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsBewertung: 4.5 von 5 Sternen4.5/5 (169)
- ADHD is Awesome: A Guide to (Mostly) Thriving with ADHDVon EverandADHD is Awesome: A Guide to (Mostly) Thriving with ADHDBewertung: 5 von 5 Sternen5/5 (1)
- Why We Die: The New Science of Aging and the Quest for ImmortalityVon EverandWhy We Die: The New Science of Aging and the Quest for ImmortalityBewertung: 4 von 5 Sternen4/5 (3)
- Gut: the new and revised Sunday Times bestsellerVon EverandGut: the new and revised Sunday Times bestsellerBewertung: 4 von 5 Sternen4/5 (392)
- The Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeVon EverandThe Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeBewertung: 4.5 von 5 Sternen4.5/5 (253)
- The Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsVon EverandThe Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsBewertung: 3.5 von 5 Sternen3.5/5 (3)
- When the Body Says No by Gabor Maté: Key Takeaways, Summary & AnalysisVon EverandWhen the Body Says No by Gabor Maté: Key Takeaways, Summary & AnalysisBewertung: 3.5 von 5 Sternen3.5/5 (2)
- Sleep Stories for Adults: Overcome Insomnia and Find a Peaceful AwakeningVon EverandSleep Stories for Adults: Overcome Insomnia and Find a Peaceful AwakeningBewertung: 4 von 5 Sternen4/5 (3)
- Dark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Von EverandDark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Bewertung: 4.5 von 5 Sternen4.5/5 (110)
- To Explain the World: The Discovery of Modern ScienceVon EverandTo Explain the World: The Discovery of Modern ScienceBewertung: 3.5 von 5 Sternen3.5/5 (51)
- An Autobiography of Trauma: A Healing JourneyVon EverandAn Autobiography of Trauma: A Healing JourneyBewertung: 5 von 5 Sternen5/5 (2)
- Mindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessVon EverandMindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessBewertung: 4.5 von 5 Sternen4.5/5 (328)
- Outlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisVon EverandOutlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisBewertung: 4 von 5 Sternen4/5 (1)
- Cult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryVon EverandCult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryBewertung: 4 von 5 Sternen4/5 (44)
- Summary: The Myth of Normal: Trauma, Illness, and Healing in a Toxic Culture By Gabor Maté MD & Daniel Maté: Key Takeaways, Summary & AnalysisVon EverandSummary: The Myth of Normal: Trauma, Illness, and Healing in a Toxic Culture By Gabor Maté MD & Daniel Maté: Key Takeaways, Summary & AnalysisBewertung: 4 von 5 Sternen4/5 (9)