Das könnte Ihnen auch gefallen
- Top Trials in Gastroenterology & HepatologyVon EverandTop Trials in Gastroenterology & HepatologyBewertung: 4.5 von 5 Sternen4.5/5 (7)
- Effect of Integrated Traditional Chinese and Western Medicine On GoutDokument11 SeitenEffect of Integrated Traditional Chinese and Western Medicine On GoutHuy PhạmNoch keine Bewertungen
- The Effect of Non-Steroidal Anti-Inflammatory Drugs On Severity of Acute Pancreatitis and Pancreatic NecrosisDokument4 SeitenThe Effect of Non-Steroidal Anti-Inflammatory Drugs On Severity of Acute Pancreatitis and Pancreatic NecrosisAracelyAcostaNoch keine Bewertungen
- 1850-Article Text-24018-2-10-20191004Dokument5 Seiten1850-Article Text-24018-2-10-20191004Hải TrầnNoch keine Bewertungen
- Peptic UlcerDokument11 SeitenPeptic UlcerdefinaNoch keine Bewertungen
- zhu2017Dokument9 Seitenzhu2017Hải TrầnNoch keine Bewertungen
- Khannasharma 2017Dokument7 SeitenKhannasharma 2017Imam IskandarNoch keine Bewertungen
- Rheumatology Kev006 FullDokument7 SeitenRheumatology Kev006 FullMajito DondioNoch keine Bewertungen
- On MedDokument10 SeitenOn MedShimily LiangNoch keine Bewertungen
- 96 303 1 PBDokument4 Seiten96 303 1 PBدحلمىالضلعNoch keine Bewertungen
- Diacerein For The Treatment of Rheumatoid Arthritis in Patients With Inadequate Response To Methotrexate A Pilot Randomized, Double-Blind, Placebo-Controlled Add-On Trial - TEM HTMLDokument11 SeitenDiacerein For The Treatment of Rheumatoid Arthritis in Patients With Inadequate Response To Methotrexate A Pilot Randomized, Double-Blind, Placebo-Controlled Add-On Trial - TEM HTMLAline Leal CortesNoch keine Bewertungen
- Zhao, 2021 PDFDokument10 SeitenZhao, 2021 PDFiaw iawNoch keine Bewertungen
- Pain Medicine 2015 16: 782-790 Wiley Periodicals, IncDokument9 SeitenPain Medicine 2015 16: 782-790 Wiley Periodicals, IncMaty LaraNoch keine Bewertungen
- Alzheimer's Disease Treated With Combined Therapy Based On NourishingDokument5 SeitenAlzheimer's Disease Treated With Combined Therapy Based On Nourishinggiovanna2004Noch keine Bewertungen
- The Review of The Yanghe Decoction About Its Clinical and Experimental ResearchDokument6 SeitenThe Review of The Yanghe Decoction About Its Clinical and Experimental Researchvender.sptzxNoch keine Bewertungen
- AcupressureDokument9 SeitenAcupressureFebi Tria KurniasariNoch keine Bewertungen
- Wa0010.Dokument9 SeitenWa0010.deinoterraNoch keine Bewertungen
- GR 08 216Dokument10 SeitenGR 08 2161110018006 NOVIA SUSANTINoch keine Bewertungen
- Randomized Controlled Trial of Transoral IncisionlessDokument13 SeitenRandomized Controlled Trial of Transoral IncisionlessResidentes CirugiaNoch keine Bewertungen
- CosentyxDokument10 SeitenCosentyxsamar RamadanNoch keine Bewertungen
- 2014-Effects and Mechanisms of Transcutaneous Electroacupuncture On Chemotherapy Induced Nausea and VomitingDokument6 Seiten2014-Effects and Mechanisms of Transcutaneous Electroacupuncture On Chemotherapy Induced Nausea and VomitingvictoregvNoch keine Bewertungen
- Kontras StatinDokument10 SeitenKontras Statinale_rhdNoch keine Bewertungen
- Early Management of Acute Pancreatitis-A Review of The Best Evidence. Dig Liver Dis 2017Dokument32 SeitenEarly Management of Acute Pancreatitis-A Review of The Best Evidence. Dig Liver Dis 2017América FloresNoch keine Bewertungen
- Analgesia en Apendicitis AgudaDokument3 SeitenAnalgesia en Apendicitis Agudasilvia barbosaNoch keine Bewertungen
- Evidence Based Clinical PracticeDokument18 SeitenEvidence Based Clinical PracticeEka RizkyanaNoch keine Bewertungen
- Medicine: Effect of Magnesium Sulfate On Renal Colic PainDokument8 SeitenMedicine: Effect of Magnesium Sulfate On Renal Colic PainJunaidy TahirNoch keine Bewertungen
- Comparison of Octreotide and Hyoscine in Controlling Gastrointestinal Symptoms Due To Malignant Inoperable Bowel ObstructionDokument4 SeitenComparison of Octreotide and Hyoscine in Controlling Gastrointestinal Symptoms Due To Malignant Inoperable Bowel ObstructionThiago GomesNoch keine Bewertungen
- Turkjmedsci-50-354 PubmedDokument6 SeitenTurkjmedsci-50-354 PubmedRizka Uda'aNoch keine Bewertungen
- Art 21054Dokument10 SeitenArt 21054Ndhy Pharm HabibieNoch keine Bewertungen
- Tofacitinib As Induction and Maintenance Therapy For Ulcerative ColitisDokument14 SeitenTofacitinib As Induction and Maintenance Therapy For Ulcerative Colitismichal ben meronNoch keine Bewertungen
- Jurnal Tatalaksana 2Dokument7 SeitenJurnal Tatalaksana 2winny kartikaNoch keine Bewertungen
- Jamainternal He 2022 Oi 220009 1648216452.48575Dokument7 SeitenJamainternal He 2022 Oi 220009 1648216452.48575Mesan KoNoch keine Bewertungen
- Effect Observation of Electro Acupunctute AnesthesiaDokument7 SeitenEffect Observation of Electro Acupunctute Anesthesiaadink mochammadNoch keine Bewertungen
- Art2 HT3Dokument3 SeitenArt2 HT3Glenda MaríaNoch keine Bewertungen
- PIIS2468125320301266Dokument12 SeitenPIIS2468125320301266Putrisuci AndytichaNoch keine Bewertungen
- NSAIDs May Delay Peptic Ulcer Healing in Rheumatic PatientsDokument4 SeitenNSAIDs May Delay Peptic Ulcer Healing in Rheumatic PatientsheldaseptivanyNoch keine Bewertungen
- Prevention of Post ERCP Pancreatitis Where Are We NowDokument5 SeitenPrevention of Post ERCP Pancreatitis Where Are We NowPaul HartingNoch keine Bewertungen
- Adverse Event Chloroquine 1Dokument8 SeitenAdverse Event Chloroquine 1Ingrid KoutioNoch keine Bewertungen
- Jama Yang 2023 Oi 230112 1697473261.42652Dokument12 SeitenJama Yang 2023 Oi 230112 1697473261.42652adol1018Noch keine Bewertungen
- Para Tradudir Ejercisios y Espondilitis AnquilosanteDokument10 SeitenPara Tradudir Ejercisios y Espondilitis AnquilosanteCarla Bocca MoralesNoch keine Bewertungen
- Clinical Outcomes of Esophagogastroduodenoscopy In.27Dokument6 SeitenClinical Outcomes of Esophagogastroduodenoscopy In.27Agung KaryawinaraNoch keine Bewertungen
- Effect of Antibiotic Prophylaxis On Acute Necrotizing Pancreatitis: Results of A Randomized Controlled TrialDokument7 SeitenEffect of Antibiotic Prophylaxis On Acute Necrotizing Pancreatitis: Results of A Randomized Controlled TrialKirsten HartmanNoch keine Bewertungen
- Effects of Low Dose Amitriptyline On Epigastric Pain Syndrome in Functional Dyspepsia PatientsDokument5 SeitenEffects of Low Dose Amitriptyline On Epigastric Pain Syndrome in Functional Dyspepsia PatientsAnnisa apriliaNoch keine Bewertungen
- 1 s2.0 S001650850862925X MainDokument2 Seiten1 s2.0 S001650850862925X MainMirza RisqaNoch keine Bewertungen
- Original Research Article: Anurag Bijalwan, Pradeep Singhal, Syed AltamashDokument7 SeitenOriginal Research Article: Anurag Bijalwan, Pradeep Singhal, Syed Altamashagus sukarnaNoch keine Bewertungen
- Proktitis 1Dokument2 SeitenProktitis 1adi chandraNoch keine Bewertungen
- Nonsteroidal Anti-Inflammatory Drug Use As A Risk Factor For Gastro-Oesophageal Reflux Disease: An Observational StudyDokument6 SeitenNonsteroidal Anti-Inflammatory Drug Use As A Risk Factor For Gastro-Oesophageal Reflux Disease: An Observational StudyGina NabilahNoch keine Bewertungen
- Comparative Clinical Trial of S-Pantoprazole Racemic Pantoprazole in The Treatment of Gastro-Esophageal Reflux DiseaseDokument4 SeitenComparative Clinical Trial of S-Pantoprazole Racemic Pantoprazole in The Treatment of Gastro-Esophageal Reflux DiseaseSiddharth SikariaNoch keine Bewertungen
- tratamiento con AINESDokument6 Seitentratamiento con AINESCarol Chávez MedinaNoch keine Bewertungen
- Fphar 13 1021584Dokument11 SeitenFphar 13 1021584topanNoch keine Bewertungen
- 10 1016@j Clinthera 2020 01 008Dokument19 Seiten10 1016@j Clinthera 2020 01 008skripsi kapNoch keine Bewertungen
- Acute Effect of Transcutaneous Electroacupuncture On Globus Pharyngeus - A Randomized, Single-Blind, Crossover Trial (ZHOU 2020)Dokument9 SeitenAcute Effect of Transcutaneous Electroacupuncture On Globus Pharyngeus - A Randomized, Single-Blind, Crossover Trial (ZHOU 2020)DANDYNoch keine Bewertungen
- Incidence and Risk Factors of Anti-Tuberculosis DRDokument11 SeitenIncidence and Risk Factors of Anti-Tuberculosis DRDi LaNoch keine Bewertungen
- 1 s2.0 S0735109716003983 MainDokument11 Seiten1 s2.0 S0735109716003983 MaintopanNoch keine Bewertungen
- Research Study JournalDokument27 SeitenResearch Study JournalHyacinth A RotaNoch keine Bewertungen
- New England Journal Medicine: The ofDokument11 SeitenNew England Journal Medicine: The ofAlvin JulianNoch keine Bewertungen
- 2011 A Randomized Controlled Trial of Laparoscopic Nissen Fundoplication Versus PPIs For The Treatment of Patients With GERDDokument8 Seiten2011 A Randomized Controlled Trial of Laparoscopic Nissen Fundoplication Versus PPIs For The Treatment of Patients With GERDResidentes Cirugia Udea 2016Noch keine Bewertungen
- SELECT-MONOTHERAPY FullDokument9 SeitenSELECT-MONOTHERAPY FullAlaitz GurreaNoch keine Bewertungen
- Research Article: Management of Amavata (Rheumatoid Arthritis) by Application of Ayurvedic PrincipleDokument6 SeitenResearch Article: Management of Amavata (Rheumatoid Arthritis) by Application of Ayurvedic PrinciplerajrajNoch keine Bewertungen
- Effectiveness of Curcuma Longa Extract For The Treatment of Symptoms and Effusion-Synovitis of Knee OsteoarthritisDokument12 SeitenEffectiveness of Curcuma Longa Extract For The Treatment of Symptoms and Effusion-Synovitis of Knee OsteoarthritisVira HeumasseNoch keine Bewertungen
- Occupational Health in Indonesia: Astrid Sulistomo Dep. of Community Medicine FmuiDokument99 SeitenOccupational Health in Indonesia: Astrid Sulistomo Dep. of Community Medicine FmuiDea MaharaniNoch keine Bewertungen
- 07e. Neoplasm of GitDokument39 Seiten07e. Neoplasm of Git21701101016 - Juliana Ayu NugrahaNoch keine Bewertungen
- NO Prodi Link Zoom No Peserta Peserta Room PukulDokument1 SeiteNO Prodi Link Zoom No Peserta Peserta Room Pukul21701101016 - Juliana Ayu NugrahaNoch keine Bewertungen
- 1 SM PDFDokument12 Seiten1 SM PDF21701101016 - Juliana Ayu NugrahaNoch keine Bewertungen
- 07a. Non Neoplastic Disease of OesophagusDokument35 Seiten07a. Non Neoplastic Disease of Oesophagus21701101016 - Juliana Ayu NugrahaNoch keine Bewertungen
- TRSLT DR Nur Helmint ProtozoaDokument26 SeitenTRSLT DR Nur Helmint Protozoa21701101016 - Juliana Ayu NugrahaNoch keine Bewertungen
- Tata Laksana Pasien dengan Kasus MultitraumaDokument104 SeitenTata Laksana Pasien dengan Kasus Multitrauma21701101016 - Juliana Ayu NugrahaNoch keine Bewertungen
- Pekerjaan Lapangan PDFDokument3 SeitenPekerjaan Lapangan PDF21701101016 - Juliana Ayu NugrahaNoch keine Bewertungen
- 5.e Brochure WBMDokument12 Seiten5.e Brochure WBM21701101016 - Juliana Ayu NugrahaNoch keine Bewertungen
- Ef Ficacy and Safety of Ginger in Osteoarthritis Patients: A Meta-Analysis of Randomized Placebo-Controlled TrialsDokument9 SeitenEf Ficacy and Safety of Ginger in Osteoarthritis Patients: A Meta-Analysis of Randomized Placebo-Controlled Trials21701101016 - Juliana Ayu NugrahaNoch keine Bewertungen
- 07c. Non Neoplastic Disease of The Small and Large IntestineDokument49 Seiten07c. Non Neoplastic Disease of The Small and Large Intestine21701101016 - Juliana Ayu NugrahaNoch keine Bewertungen
- Histology DigestiveDokument18 SeitenHistology Digestive21701101016 - Juliana Ayu NugrahaNoch keine Bewertungen
- Nutri SiDokument9 SeitenNutri Si21701101016 - Juliana Ayu NugrahaNoch keine Bewertungen
- Nutrisi PDFDokument85 SeitenNutrisi PDF21701101016 - Juliana Ayu NugrahaNoch keine Bewertungen
- DR Dini Sri Damayanti, MkesDokument48 SeitenDR Dini Sri Damayanti, Mkes21701101016 - Juliana Ayu NugrahaNoch keine Bewertungen
- Fisiologi Pengaturan Tekanan Darah SILBERNAGL 2Dokument6 SeitenFisiologi Pengaturan Tekanan Darah SILBERNAGL 221701101016 - Juliana Ayu NugrahaNoch keine Bewertungen
- Who Seeks Alternative Health Care? A Profile of The Users of Five Modes of TreatmentDokument14 SeitenWho Seeks Alternative Health Care? A Profile of The Users of Five Modes of TreatmentEdward Joshua NuguidNoch keine Bewertungen
- Shen-Atlas of AcupunctureDokument256 SeitenShen-Atlas of AcupunctureMiguel A Cordero100% (1)
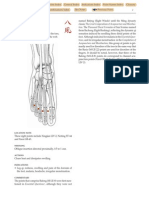
- BAFENG (M-LE-8) : Eight WindsDokument1 SeiteBAFENG (M-LE-8) : Eight Windsray72roNoch keine Bewertungen
- Chakras e AcupunturaDokument6 SeitenChakras e AcupunturaVitor Caruso100% (1)
- Research Article: Effects of Electroacupuncture at BL60 On Formalin-Induced Pain in RatsDokument7 SeitenResearch Article: Effects of Electroacupuncture at BL60 On Formalin-Induced Pain in RatsocoxodoNoch keine Bewertungen
- Aguja HinashinDokument6 SeitenAguja HinashinFernando IglesiasNoch keine Bewertungen
- Accupressure POINTSDokument22 SeitenAccupressure POINTSsupportNoch keine Bewertungen
- Sa-Ahm Five Element Acupuncture PDFDokument12 SeitenSa-Ahm Five Element Acupuncture PDFlashmiNoch keine Bewertungen
- Guide to Auriculotherapy Treatment ProceduresDokument30 SeitenGuide to Auriculotherapy Treatment ProceduresIkshitNoch keine Bewertungen
- Class 5 Notes - DR Tan's Balancing MethodDokument7 SeitenClass 5 Notes - DR Tan's Balancing Methodfuzzface23100% (20)
- AcupuncturePointCompendium2014 PDFDokument269 SeitenAcupuncturePointCompendium2014 PDFlinecurNoch keine Bewertungen
- Lecturas InglesDokument9 SeitenLecturas Ingleslee47Noch keine Bewertungen
- Acu TonicsDokument13 SeitenAcu TonicsCarlo Damião100% (3)
- The Journal of Chinese Medicine and AcupunctureDokument56 SeitenThe Journal of Chinese Medicine and Acupuncturemartin sandaNoch keine Bewertungen
- Gateway B2 Test 6A 1-3 PDFDokument3 SeitenGateway B2 Test 6A 1-3 PDFlourdes100% (1)
- Fascia, Meridians & Trigger Points: Exploring ConnectionsDokument4 SeitenFascia, Meridians & Trigger Points: Exploring ConnectionsNaresh MuttavarapuNoch keine Bewertungen
- MAPEH - HealthDokument3 SeitenMAPEH - HealthALLISONNoch keine Bewertungen
- Placebo Studies Ritual TheoryDokument10 SeitenPlacebo Studies Ritual Theoryapi-443830029Noch keine Bewertungen
- Intro To Scalp Acupuncture - 25 Pages PDFDokument25 SeitenIntro To Scalp Acupuncture - 25 Pages PDFafisioterapia100% (5)
- Cutaneous Part of MeridiansDokument3 SeitenCutaneous Part of MeridiansdevabakhtiNoch keine Bewertungen
- Microneedling 2019Dokument5 SeitenMicroneedling 2019danielagonzalezt5100% (2)
- Health & Fitness UK - August 2019Dokument100 SeitenHealth & Fitness UK - August 2019Phubinh ChemicalNoch keine Bewertungen
- BFA FullDokument9 SeitenBFA Fullhistory APNoch keine Bewertungen
- 1992-2007 KPDS PARAGRAF TAMAMLAMA SORULARI (39Dokument36 Seiten1992-2007 KPDS PARAGRAF TAMAMLAMA SORULARI (39ahmet parlakNoch keine Bewertungen
- Journal of Acpuncture and Tuina Science, Apr. 2005. Vol.3, No.2Dokument62 SeitenJournal of Acpuncture and Tuina Science, Apr. 2005. Vol.3, No.2Mayra Elizabeth Castillo ArruèNoch keine Bewertungen
- Edward Eagan's achievements at Summer and Winter OlympicsDokument9 SeitenEdward Eagan's achievements at Summer and Winter OlympicsLinh CottonNoch keine Bewertungen
- Back Pain by Martin Arrowsmith PDFDokument49 SeitenBack Pain by Martin Arrowsmith PDFEd BegsNoch keine Bewertungen
- F.C.E TIPS & PRACTICEDokument22 SeitenF.C.E TIPS & PRACTICEAlina TeranNoch keine Bewertungen
- Acupuncture Points For Beginners - The Science Behind How Acupuncture Helps Relieve PainDokument103 SeitenAcupuncture Points For Beginners - The Science Behind How Acupuncture Helps Relieve PainMaggie50% (2)
- AcupointsDokument13 SeitenAcupointspeter911x100% (1)