Das könnte Ihnen auch gefallen
- Differential Diagnosis of Late-Type Reactions To Injected Local Anaesthetics, Inflammation at The Injection Site Is The Only Indicator of Allergic HypersensitivityDokument7 SeitenDifferential Diagnosis of Late-Type Reactions To Injected Local Anaesthetics, Inflammation at The Injection Site Is The Only Indicator of Allergic HypersensitivityPatricia AndradeNoch keine Bewertungen
- Appropiate Allergic Testing and The Interpretation - Dr. Deshinta Putri Mulya, SP - PD (K) KAIDokument40 SeitenAppropiate Allergic Testing and The Interpretation - Dr. Deshinta Putri Mulya, SP - PD (K) KAIEllenNoch keine Bewertungen
- Iagnóstico Diferencial de Reacciones de Tipo Tardío A Anestésicos Locales InyectadosDokument7 SeitenIagnóstico Diferencial de Reacciones de Tipo Tardío A Anestésicos Locales Inyectadosmrestrepo55501Noch keine Bewertungen
- allergic testสถาบัน Hondout ดร.พญ.จงกลนี PDFDokument26 Seitenallergic testสถาบัน Hondout ดร.พญ.จงกลนี PDFThiti JessadaromNoch keine Bewertungen
- Bio AllergyDokument7 SeitenBio AllergyShashwat YadavNoch keine Bewertungen
- Allergic Rhinitis Slides 070926 PDFDokument57 SeitenAllergic Rhinitis Slides 070926 PDFmhamad kabraNoch keine Bewertungen
- Trend in Laboratory Diagnostic For AllergyDokument29 SeitenTrend in Laboratory Diagnostic For Allergygonteng sadyogaNoch keine Bewertungen
- PHCP Lec Week 1 Respiratory DisordersDokument15 SeitenPHCP Lec Week 1 Respiratory DisorderslarissalieveNoch keine Bewertungen
- Specific Ige (Allergy) Tests: Page 1 of 2Dokument2 SeitenSpecific Ige (Allergy) Tests: Page 1 of 2tersiaNoch keine Bewertungen
- Photosensitivity Test (Chapter 13) : Go Back To The TopDokument4 SeitenPhotosensitivity Test (Chapter 13) : Go Back To The TopjordyNoch keine Bewertungen
- SkinTesting BeforeAntibiotic Administration Is There A Scientific BasisDokument3 SeitenSkinTesting BeforeAntibiotic Administration Is There A Scientific Basiskamari mohamedNoch keine Bewertungen
- Skin Testing Before Antibiotic Administration Is There A Scientific BasisDokument3 SeitenSkin Testing Before Antibiotic Administration Is There A Scientific Basiskamari mohamedNoch keine Bewertungen
- Prelims - GMJ RLE - Module 2 III DisorderDokument4 SeitenPrelims - GMJ RLE - Module 2 III DisorderjuiceNoch keine Bewertungen
- Drug Allergy: Penicillin, Aspirin and Sulfa DrugsDokument87 SeitenDrug Allergy: Penicillin, Aspirin and Sulfa Drugskarenchong938520Noch keine Bewertungen
- Seminar WordDokument32 SeitenSeminar Wordslmnkhn1988Noch keine Bewertungen
- IS.6 HypersensitivityDokument4 SeitenIS.6 HypersensitivityDANIELLA LOMA CAPONPONNoch keine Bewertungen
- Allergy: An Overview: Salwa Hassan TeamaDokument7 SeitenAllergy: An Overview: Salwa Hassan TeamaWulan YuwitaNoch keine Bewertungen
- Alergia e Anestesia COA2011Dokument6 SeitenAlergia e Anestesia COA2011Maisa RibeiroNoch keine Bewertungen
- Atopy Treatment in DogsDokument4 SeitenAtopy Treatment in DogsOzkar JaraNoch keine Bewertungen
- Hypersensitivity NotesDokument7 SeitenHypersensitivity NotesShaii Whomewhat GuyguyonNoch keine Bewertungen
- HypersensitivityDokument85 SeitenHypersensitivityAlina LubnaNoch keine Bewertungen
- Fitzpatrick's Dermatology in General Medicine, Eighth Edition, 2 Volume SetDokument30 SeitenFitzpatrick's Dermatology in General Medicine, Eighth Edition, 2 Volume SetDellNoch keine Bewertungen
- Do Not Copy: Skin Testing in AllergyDokument3 SeitenDo Not Copy: Skin Testing in AllergyHusni mubarakNoch keine Bewertungen
- AllergyDokument23 SeitenAllergyAmbl GeronNoch keine Bewertungen
- Pemeriksaan Penunjang 1. Skin Testing For Detection of Allergen-Specific IgeDokument7 SeitenPemeriksaan Penunjang 1. Skin Testing For Detection of Allergen-Specific Igerosalia puspitajayaNoch keine Bewertungen
- Dr. Khairiyadi, M.Kes., Sp.A Departemen Ilmu Kesehatan Anak RSUD Ulin BanjarmasinDokument78 SeitenDr. Khairiyadi, M.Kes., Sp.A Departemen Ilmu Kesehatan Anak RSUD Ulin BanjarmasinEldhaNoch keine Bewertungen
- cln64 4p373Dokument2 Seitencln64 4p373CT DAMNoch keine Bewertungen
- Diagnostics of AllergiesDokument20 SeitenDiagnostics of AllergiesPaola ViñéNoch keine Bewertungen
- AtopyDokument14 SeitenAtopyTooba NaeemNoch keine Bewertungen
- Piis0091674909015644 PDFDokument13 SeitenPiis0091674909015644 PDFanka_mihaelaNoch keine Bewertungen
- AllergyDokument86 SeitenAllergyhoor e ainNoch keine Bewertungen
- IS Lab Modules ReviewerDokument4 SeitenIS Lab Modules ReviewerMarie MontemarNoch keine Bewertungen
- Atopy Patch Test.Dokument4 SeitenAtopy Patch Test.KuldeepSinghBanaNoch keine Bewertungen
- Immunologic Disorder Day 3 (AutoRecovered)Dokument3 SeitenImmunologic Disorder Day 3 (AutoRecovered)IRISH CHEEN PARREÑO NACIONALNoch keine Bewertungen
- Assessment and Management of Patient's With Allergic ReactionsDokument13 SeitenAssessment and Management of Patient's With Allergic ReactionsLau ColastreNoch keine Bewertungen
- Alergia Inmunologia 2.0Dokument7 SeitenAlergia Inmunologia 2.0Antonio RONoch keine Bewertungen
- Skin Prick Testing Guide For GPs NPLDokument5 SeitenSkin Prick Testing Guide For GPs NPLniyatihopesNoch keine Bewertungen
- Patch TestDokument7 SeitenPatch TestCocea MihaiNoch keine Bewertungen
- AllergiesDokument4 SeitenAllergiesPerl AngelicNoch keine Bewertungen
- 2006 AllergyDokument9 Seiten2006 AllergyJUAN BENITO SUAREZ PALACIOSNoch keine Bewertungen
- HypersensitivityDokument59 SeitenHypersensitivityGlenn SampayanNoch keine Bewertungen
- Drug Allergy: Divya Seth, MD and Deepak Kamat, MD, PHDDokument7 SeitenDrug Allergy: Divya Seth, MD and Deepak Kamat, MD, PHDHusni mubarakNoch keine Bewertungen
- Lesson 3 Adr ClassificationDokument3 SeitenLesson 3 Adr ClassificationVincent Joshua TriboNoch keine Bewertungen
- Diagnosis & Management of Drug Allergy: Dr. Wistiani, Msi Med, Spa (K)Dokument41 SeitenDiagnosis & Management of Drug Allergy: Dr. Wistiani, Msi Med, Spa (K)Nadia Chairunnisa100% (1)
- IDflu LeafletDokument28 SeitenIDflu LeafletEllaNoch keine Bewertungen
- Drug AllergyDokument28 SeitenDrug AllergyVicky Sandhu100% (1)
- Skin TestDokument23 SeitenSkin TestpraptiwiNoch keine Bewertungen
- ASCIA HP SPT Guide 2020Dokument22 SeitenASCIA HP SPT Guide 2020Edy NoveryNoch keine Bewertungen
- PDF TJP 2372Dokument14 SeitenPDF TJP 2372Talaat OmranNoch keine Bewertungen
- Latex Allergy: Clinical Manifestations Assessment & Diagnostic Findings Medical Management Nursing ManagementDokument7 SeitenLatex Allergy: Clinical Manifestations Assessment & Diagnostic Findings Medical Management Nursing Managementjoyrena ochondraNoch keine Bewertungen
- IMMUNOLOGYDokument11 SeitenIMMUNOLOGYKiran ShahNoch keine Bewertungen
- Allergic Reactions: Ahmad Asraf Bin AmirullahDokument28 SeitenAllergic Reactions: Ahmad Asraf Bin Amirullahasraf amirullahNoch keine Bewertungen
- Peranan Antihistamin Pada Alergi Obat: Tjok - Istri Anom SaturtiDokument16 SeitenPeranan Antihistamin Pada Alergi Obat: Tjok - Istri Anom SaturtiarisuyandiNoch keine Bewertungen
- Drug AllergyDokument27 SeitenDrug AllergyqooqoowkdNoch keine Bewertungen
- MS Finals HypersensitivityDokument16 SeitenMS Finals HypersensitivityMutya XDNoch keine Bewertungen
- 06 198vertigoDokument3 Seiten06 198vertigoCahyoAjiPamungkasNoch keine Bewertungen
- Nursing Care of Clients With Allergic DisordersDokument12 SeitenNursing Care of Clients With Allergic Disordersbwee bweeNoch keine Bewertungen
- The Allergenic Activity and Clinical Impact of IndDokument31 SeitenThe Allergenic Activity and Clinical Impact of IndEverton MonteiroNoch keine Bewertungen
- Anaphylactic Reactions in Anesthesia and Intensive CareVon EverandAnaphylactic Reactions in Anesthesia and Intensive CareNoch keine Bewertungen
- The Perfect Egg Allergy Diet Cookbook:The Complete Nutrition Guide For Treating And Managing Symptoms Of Egg Allergy With Delectable And Nourishing RecipesVon EverandThe Perfect Egg Allergy Diet Cookbook:The Complete Nutrition Guide For Treating And Managing Symptoms Of Egg Allergy With Delectable And Nourishing RecipesNoch keine Bewertungen
- Anatomy of Larynx: Three Are Single (Thyroid, Cricoid, and Epiglottic)Dokument2 SeitenAnatomy of Larynx: Three Are Single (Thyroid, Cricoid, and Epiglottic)Nazmun LailahNoch keine Bewertungen
- Description Dermatological StatusDokument6 SeitenDescription Dermatological StatusNazmun LailahNoch keine Bewertungen
- Anatomy of Breast: Thoracic Aorta in The 2nd, 3rd, and 4th Intercostal SpacesDokument4 SeitenAnatomy of Breast: Thoracic Aorta in The 2nd, 3rd, and 4th Intercostal SpacesNazmun LailahNoch keine Bewertungen
- Abdominal Pain: No. Features Explanation Associated WithDokument4 SeitenAbdominal Pain: No. Features Explanation Associated WithNazmun LailahNoch keine Bewertungen
- HemostasisDokument1 SeiteHemostasisNazmun LailahNoch keine Bewertungen
- Control of ErythropoiesisDokument13 SeitenControl of ErythropoiesisNazmun LailahNoch keine Bewertungen
- General Properties of VirusDokument4 SeitenGeneral Properties of VirusNazmun LailahNoch keine Bewertungen
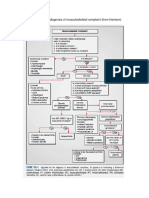
- Algorithm For The Diagnosis of Musculoskeletal ComplaintDokument1 SeiteAlgorithm For The Diagnosis of Musculoskeletal ComplaintNazmun LailahNoch keine Bewertungen
- WWWDokument66 SeitenWWWNazmun LailahNoch keine Bewertungen
- Child TB Training Toolkit WebDokument47 SeitenChild TB Training Toolkit WebAsena TuiketeiNoch keine Bewertungen
- Hygiene Sanitation and WaterDokument9 SeitenHygiene Sanitation and WaterNazmun LailahNoch keine Bewertungen
- Preventing Disease Through Healthy Environments: Towards An Estimate of The Environmental Burden of DiseaseDokument16 SeitenPreventing Disease Through Healthy Environments: Towards An Estimate of The Environmental Burden of DiseaseNazmun LailahNoch keine Bewertungen
- Telfast Product PresentationDokument32 SeitenTelfast Product PresentationDewi Sri NuritaNoch keine Bewertungen
- HypersensivityDokument18 SeitenHypersensivityJessica TieuNoch keine Bewertungen
- Ulcerative ColitisDokument18 SeitenUlcerative ColitisHoussein EL HajjNoch keine Bewertungen
- Conjunctivitis CaseDokument6 SeitenConjunctivitis CaseSuhas IngaleNoch keine Bewertungen
- ERITRODERMADokument28 SeitenERITRODERMASariAzisyaNoch keine Bewertungen
- Effectiveness and Pharmacoeconomic Analysis of The Treatment of Severe Asthma With Omalizumab in Clinical PracticeDokument9 SeitenEffectiveness and Pharmacoeconomic Analysis of The Treatment of Severe Asthma With Omalizumab in Clinical PracticePetrus Kabul TogarmaNoch keine Bewertungen
- ALSANGEDY BULLETS FOR PACES Angioedema 2nd Edition PDFDokument2 SeitenALSANGEDY BULLETS FOR PACES Angioedema 2nd Edition PDFushapadminivadivelswamyNoch keine Bewertungen
- Autoimmune Bullous Diseases Associations: Suzana Ljubojevic, MD, PHD, Jasna Lipozen Čić, MD, PHDDokument17 SeitenAutoimmune Bullous Diseases Associations: Suzana Ljubojevic, MD, PHD, Jasna Lipozen Čić, MD, PHDRunuk BhandariNoch keine Bewertungen
- Autoimmune DiseaseDokument3 SeitenAutoimmune DiseasePearl AudeNoch keine Bewertungen
- PIIS0091674911015594Dokument6 SeitenPIIS0091674911015594danaagus81Noch keine Bewertungen
- Atlas of Immunofluorescence in Dermatology, Mayo Clinic - KalaajiDokument86 SeitenAtlas of Immunofluorescence in Dermatology, Mayo Clinic - KalaajiDana ȘerbanNoch keine Bewertungen
- Hanifin and Rajka Diagnostic Criteria For Atopic DermatitisDokument3 SeitenHanifin and Rajka Diagnostic Criteria For Atopic DermatitisAlief LeisyahNoch keine Bewertungen
- Nummular EczemaDokument1 SeiteNummular EczemaCitra AnandiraNoch keine Bewertungen
- Group 5 Document-1Dokument8 SeitenGroup 5 Document-1noumantamilNoch keine Bewertungen
- Hypersensitivity Reaction/ AllergyDokument23 SeitenHypersensitivity Reaction/ AllergyCharity Grace MagnoNoch keine Bewertungen
- DERMATITISDokument2 SeitenDERMATITISKevinJuliusTanadyNoch keine Bewertungen
- Chung 2014Dokument6 SeitenChung 2014Retno ManggalihNoch keine Bewertungen
- Blistering DiseasesDokument26 SeitenBlistering DiseasesLia-Maria BufteaNoch keine Bewertungen
- Analisis Spasial Penyakit Dermatitis Di Puskesmas Labakkang Kabupaten PangkepDokument8 SeitenAnalisis Spasial Penyakit Dermatitis Di Puskesmas Labakkang Kabupaten PangkepfifidianNoch keine Bewertungen
- 1 s2.0 S1474442222004318 MainDokument15 Seiten1 s2.0 S1474442222004318 MainItamar MeirelesNoch keine Bewertungen
- PemphigusDokument15 SeitenPemphigusMelly Narzabal100% (1)
- ThalaiTe Inleng NOVEMBERDokument4 SeitenThalaiTe Inleng NOVEMBERLalmuansanga Chhakchhuak StcNoch keine Bewertungen
- AtopyDokument5 SeitenAtopyAbdusSomadNoch keine Bewertungen
- 3.2.2.3 Penyakit AutoimunDokument64 Seiten3.2.2.3 Penyakit AutoimunKhairani HakimNoch keine Bewertungen
- Ana TestDokument4 SeitenAna TestFariz NurNoch keine Bewertungen
- AutoimmunityDokument40 SeitenAutoimmunityKarl RobleNoch keine Bewertungen
- Daftar PustakaDokument3 SeitenDaftar PustakalenaarfahNoch keine Bewertungen
- BULLOUS PEMPHIGOID-anto-1Dokument21 SeitenBULLOUS PEMPHIGOID-anto-1Nur RifqahNoch keine Bewertungen
- Autoimmune Diseases: Dr. Ansar Uddin Ahmed Asst. Prof and Head Dept. of Periodontology and Oral PathologyDokument13 SeitenAutoimmune Diseases: Dr. Ansar Uddin Ahmed Asst. Prof and Head Dept. of Periodontology and Oral PathologyTas DidNoch keine Bewertungen
- Anki Derm 2Dokument4 SeitenAnki Derm 2Simran SandhuNoch keine Bewertungen