Das könnte Ihnen auch gefallen
- Anatomy of Larynx: Three Are Single (Thyroid, Cricoid, and Epiglottic)Dokument2 SeitenAnatomy of Larynx: Three Are Single (Thyroid, Cricoid, and Epiglottic)Nazmun LailahNoch keine Bewertungen
- Anatomy of Breast: Thoracic Aorta in The 2nd, 3rd, and 4th Intercostal SpacesDokument4 SeitenAnatomy of Breast: Thoracic Aorta in The 2nd, 3rd, and 4th Intercostal SpacesNazmun LailahNoch keine Bewertungen
- Abdominal Pain: No. Features Explanation Associated WithDokument4 SeitenAbdominal Pain: No. Features Explanation Associated WithNazmun LailahNoch keine Bewertungen
- Description Dermatological StatusDokument6 SeitenDescription Dermatological StatusNazmun LailahNoch keine Bewertungen
- Purpose: Indication:: Material and Procedures: Patch Testing Involves TheDokument2 SeitenPurpose: Indication:: Material and Procedures: Patch Testing Involves TheNazmun LailahNoch keine Bewertungen
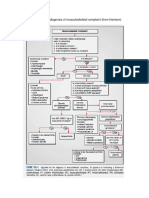
- Algorithm For The Diagnosis of Musculoskeletal ComplaintDokument1 SeiteAlgorithm For The Diagnosis of Musculoskeletal ComplaintNazmun LailahNoch keine Bewertungen
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (400)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (345)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (74)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2259)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (121)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- DNA RNA WorksheetDokument5 SeitenDNA RNA WorksheetKathleen FrancoNoch keine Bewertungen
- Jay Tugend - Protein Synthesis Performance TaskDokument7 SeitenJay Tugend - Protein Synthesis Performance Taskapi-673971695Noch keine Bewertungen
- BIO2107 - Tutorial 4 Discussion PointsDokument4 SeitenBIO2107 - Tutorial 4 Discussion PointsAjay Sookraj RamgolamNoch keine Bewertungen
- Cell Processes: Photosynthesis and Cellular RespirationDokument2 SeitenCell Processes: Photosynthesis and Cellular RespirationSecret SantaNoch keine Bewertungen
- Class 12 Respiration NotesDokument13 SeitenClass 12 Respiration NotesBrindhaVasudevan0% (1)
- LaudabletasksDokument25 SeitenLaudabletasksiremsenakNoch keine Bewertungen
- 2012 A Level Answers P1 and P2 Compiled FinalDokument12 Seiten2012 A Level Answers P1 and P2 Compiled FinalWesley TanNoch keine Bewertungen
- Aerobic Respiration Power PointDokument35 SeitenAerobic Respiration Power PointJeremy WongNoch keine Bewertungen
- Cell Energy SEDokument6 SeitenCell Energy SEArt LoversNoch keine Bewertungen
- Enzyme RegulationDokument9 SeitenEnzyme RegulationKanchi100% (1)
- The Cellular Basis of Reproduction and Inheritance: Powerpoint Lectures ForDokument66 SeitenThe Cellular Basis of Reproduction and Inheritance: Powerpoint Lectures ForLeah TibbetsNoch keine Bewertungen
- General Translation MechanismDokument15 SeitenGeneral Translation MechanismAishwarya KashyapNoch keine Bewertungen
- Kendriya VidyalayaDokument10 SeitenKendriya VidyalayaVanshNoch keine Bewertungen
- Manual xf24 Cell Mito Stress Test KitDokument47 SeitenManual xf24 Cell Mito Stress Test KitSusan HsiaoNoch keine Bewertungen
- Bio Q2 ReviewerDokument10 SeitenBio Q2 Reviewerapril LomocsoNoch keine Bewertungen
- Neurochemical Aspects of Traumatic and Neurodegenerative DiseasesDokument414 SeitenNeurochemical Aspects of Traumatic and Neurodegenerative Diseasesdra. yalithNoch keine Bewertungen
- Las Q4 Week-2 GenDokument8 SeitenLas Q4 Week-2 GenFranzhean Balais CuachonNoch keine Bewertungen
- How Cells Harvest Energy: Life Is Driven by EnergyDokument24 SeitenHow Cells Harvest Energy: Life Is Driven by EnergyNasreen MinNoch keine Bewertungen
- Na Mlbio Ch11Dokument36 SeitenNa Mlbio Ch11Life with CourteneyNoch keine Bewertungen
- A Literature-Based Review and Docking Study Emphasized On Its Anticancer Mechanisms of CarvacrolDokument13 SeitenA Literature-Based Review and Docking Study Emphasized On Its Anticancer Mechanisms of CarvacrolArifur Rahman TanzilNoch keine Bewertungen
- McKee Chapter8 Sample PDFDokument44 SeitenMcKee Chapter8 Sample PDFMustafa Kırca100% (1)
- Summative Test in Biotechnology First Quarter Name: - Section: - Score: - Multiple ChoiceDokument2 SeitenSummative Test in Biotechnology First Quarter Name: - Section: - Score: - Multiple Choicejimbo0988% (8)
- Chemistry of Signals and ReceptorsDokument13 SeitenChemistry of Signals and Receptorsour lectureNoch keine Bewertungen
- Thyroid Hormone Regulation of Metabolism: Rashmi Mullur, Yan-Yun Liu, and Gregory A. BrentDokument29 SeitenThyroid Hormone Regulation of Metabolism: Rashmi Mullur, Yan-Yun Liu, and Gregory A. BrentNissa SissariNoch keine Bewertungen
- Fatty Acid MetabolismDokument28 SeitenFatty Acid MetabolismMitchelle SaurambaNoch keine Bewertungen
- The Are in The For: BIOL 220 - Final (Page 1)Dokument14 SeitenThe Are in The For: BIOL 220 - Final (Page 1)Jad AwadNoch keine Bewertungen
- Epigenomics: What Is The Epigenome?Dokument2 SeitenEpigenomics: What Is The Epigenome?Sri Harsha SappaNoch keine Bewertungen
- 6 BIO462 Chapter 6Dokument21 Seiten6 BIO462 Chapter 6Syafiqah SuhaimiNoch keine Bewertungen
- Must Review ThisDokument19 SeitenMust Review Thispmp123456Noch keine Bewertungen
- MTPC 140: Molecular Biology and DiagnosticsDokument40 SeitenMTPC 140: Molecular Biology and DiagnosticsValdez Francis ZaccheauNoch keine Bewertungen