Das könnte Ihnen auch gefallen
- Complementary and Alternative Medical Lab Testing Part 14: ImmunologyVon EverandComplementary and Alternative Medical Lab Testing Part 14: ImmunologyNoch keine Bewertungen
- NutritionDokument10 SeitenNutritionDani ursNoch keine Bewertungen
- Investigations On Serum Lipid Profile in Patients With Urinary Tract InfectionsDokument3 SeitenInvestigations On Serum Lipid Profile in Patients With Urinary Tract InfectionsJOHNKENNEDY NNODIMNoch keine Bewertungen
- Cheng 2012 MS and Insulin Resistance As Risk Factors For Development of Chronic Kidney Disease and Rapid Decline Inrenal Function in ElderlyDokument9 SeitenCheng 2012 MS and Insulin Resistance As Risk Factors For Development of Chronic Kidney Disease and Rapid Decline Inrenal Function in ElderlyPaul SimononNoch keine Bewertungen
- 2023.5 Regional Variations of Cardiovascular Risk in Gout PatientsDokument13 Seiten2023.5 Regional Variations of Cardiovascular Risk in Gout Patientsindream81Noch keine Bewertungen
- Relationship Between C-Reactive Protein, White Blood Cell Count and Metabolic Syndrome in Nigerians With Type 2 Diabetes MellitusDokument11 SeitenRelationship Between C-Reactive Protein, White Blood Cell Count and Metabolic Syndrome in Nigerians With Type 2 Diabetes MellitusPaul Gesswein FonatabaNoch keine Bewertungen
- TurkJPhysMedRehab 65 132Dokument7 SeitenTurkJPhysMedRehab 65 132Imam IskandarNoch keine Bewertungen
- Comorbidities in Patients With Gout in R f99b8513Dokument3 SeitenComorbidities in Patients With Gout in R f99b8513Natasya SaraswatiNoch keine Bewertungen
- 7842Dokument2 Seiten7842Joseph NathanNoch keine Bewertungen
- Ijcem0007 2258Dokument8 SeitenIjcem0007 2258Nico IonaşcuNoch keine Bewertungen
- Diabetes & Metabolic Syndrome: Clinical Research & ReviewsDokument7 SeitenDiabetes & Metabolic Syndrome: Clinical Research & ReviewsMarco Antonio Guardamino OjedaNoch keine Bewertungen
- Elevated Circulating Microrna-122 Is Associated With Obesity and Insulin Resistance in Young AdultsDokument10 SeitenElevated Circulating Microrna-122 Is Associated With Obesity and Insulin Resistance in Young AdultsbushraNoch keine Bewertungen
- Joim 12743Dokument17 SeitenJoim 12743noviNoch keine Bewertungen
- Nutritional Status and Malnutrition Prevalence Among Maintenance Hemodialysis PatientsDokument8 SeitenNutritional Status and Malnutrition Prevalence Among Maintenance Hemodialysis PatientsIOSRjournalNoch keine Bewertungen
- Association Between Metabolic Syndrome and Risk of Cardiovascular Disease, Using Different Criteria and Stratified by SexDokument5 SeitenAssociation Between Metabolic Syndrome and Risk of Cardiovascular Disease, Using Different Criteria and Stratified by SexAlfredoNoch keine Bewertungen
- Tumor Necrosis Factor (TNF-α) and C-reactive Protein (CRP) are Positively Associated with the Risk of Chronic Kidney Disease in Patients with Type 2 DiabetesDokument7 SeitenTumor Necrosis Factor (TNF-α) and C-reactive Protein (CRP) are Positively Associated with the Risk of Chronic Kidney Disease in Patients with Type 2 DiabetesTea AgungNoch keine Bewertungen
- Research ArticleDokument9 SeitenResearch ArticlemikeNoch keine Bewertungen
- Falls in Patients With Liver CirrhosisDokument5 SeitenFalls in Patients With Liver CirrhosisJoana LazcurainNoch keine Bewertungen
- Metabolic Syndrome and Quality of Life in The Elderly: Age and Gender DifferencesDokument10 SeitenMetabolic Syndrome and Quality of Life in The Elderly: Age and Gender DifferencesThalia KarampasiNoch keine Bewertungen
- Prevalence of Upper GI-Endoscopic Lesions in CKDDokument7 SeitenPrevalence of Upper GI-Endoscopic Lesions in CKDheba.barkasiehNoch keine Bewertungen
- Erectile FactorDokument6 SeitenErectile FactorRidha MardiyaniNoch keine Bewertungen
- Journal of Clinical & Translational Endocrinology: SciencedirectDokument9 SeitenJournal of Clinical & Translational Endocrinology: SciencedirectidiNoch keine Bewertungen
- Impact of Serological and Histological Factors On Neurological Manifestations in Children and Adults With Celiac DiseaseDokument10 SeitenImpact of Serological and Histological Factors On Neurological Manifestations in Children and Adults With Celiac Diseaseمودة المنعميNoch keine Bewertungen
- Evaluation of The Efficiency of Bisphosphonates in The Treatment of Osteoporosis in The Climacteric PeriodDokument14 SeitenEvaluation of The Efficiency of Bisphosphonates in The Treatment of Osteoporosis in The Climacteric Periodindex PubNoch keine Bewertungen
- Cupisti2017 Article AssessmentOfPhysicalActivityCaDokument8 SeitenCupisti2017 Article AssessmentOfPhysicalActivityCanuvitaNoch keine Bewertungen
- Paper 2012Dokument13 SeitenPaper 2012Igora HernaízNoch keine Bewertungen
- Comparative Studies of Diabetes in Adult Nigerians Lipid Profile and Antioxidants Vitamins A and CDokument5 SeitenComparative Studies of Diabetes in Adult Nigerians Lipid Profile and Antioxidants Vitamins A and CEditor IJTSRDNoch keine Bewertungen
- METs DXDokument7 SeitenMETs DXมงคล ยิ่งรุ่งเรืองNoch keine Bewertungen
- 1 s2.0 S1051227619300020 MainDokument9 Seiten1 s2.0 S1051227619300020 MainRomário de Macedo EspíndolaNoch keine Bewertungen
- Risk Factors Associated With Type 2 Diabetes Mellitus and The Frequency of Nafld Affected PatientsDokument5 SeitenRisk Factors Associated With Type 2 Diabetes Mellitus and The Frequency of Nafld Affected PatientsIJAR JOURNALNoch keine Bewertungen
- Seite 92-98 #220341-ErkanDokument7 SeitenSeite 92-98 #220341-Erkancaydin33Noch keine Bewertungen
- Journal Pone 0267053Dokument10 SeitenJournal Pone 0267053Kevin TandartoNoch keine Bewertungen
- Case Report: Reynolds SyndromeDokument2 SeitenCase Report: Reynolds SyndromePeertechz Publications Inc.Noch keine Bewertungen
- Rheumatic Manifestations of Inflammatory Bowel Diseases: A Study From The Middle EastDokument11 SeitenRheumatic Manifestations of Inflammatory Bowel Diseases: A Study From The Middle EastAndreiMunteanuNoch keine Bewertungen
- Lifestyle Modifications and Erectile Dysfunction: What Can Be Expected?Dokument6 SeitenLifestyle Modifications and Erectile Dysfunction: What Can Be Expected?ANoch keine Bewertungen
- DR T Dinesh Guide DR Baba YelkeDokument27 SeitenDR T Dinesh Guide DR Baba YelkeDinesh AshwinNoch keine Bewertungen
- Gluten Free Diet Study On Celiac DiseaseDokument9 SeitenGluten Free Diet Study On Celiac DiseaseJahson WillnotloseNoch keine Bewertungen
- Vitamin D Deficiency in Patients With Active Systemic Lupus ErythematosusDokument7 SeitenVitamin D Deficiency in Patients With Active Systemic Lupus ErythematosusGeral Rocha CorrealNoch keine Bewertungen
- Handgrip Strength Stratifies The Risk of Covert and Overt Hepatic Encephalopathy in Patients With CirrhosisDokument39 SeitenHandgrip Strength Stratifies The Risk of Covert and Overt Hepatic Encephalopathy in Patients With CirrhosisAlfan FathoniNoch keine Bewertungen
- Journal Pone 0248856Dokument15 SeitenJournal Pone 0248856raihannah othmanNoch keine Bewertungen
- Wespes Et Al. Eur Urol 2006-49-806 815. EAU Guidelines On Erectile Dysfunction An UpdateDokument10 SeitenWespes Et Al. Eur Urol 2006-49-806 815. EAU Guidelines On Erectile Dysfunction An UpdateNur AnindyaNoch keine Bewertungen
- 29926539: Body Mass Index As A Predictor of Acute Kidney Injury in Critically Ill Patients A Retrospective Single-Center StudyDokument8 Seiten29926539: Body Mass Index As A Predictor of Acute Kidney Injury in Critically Ill Patients A Retrospective Single-Center StudyEward Rod SalNoch keine Bewertungen
- 1 s2.0 S1051227616301789 MainDokument7 Seiten1 s2.0 S1051227616301789 MainResearch OfficeNoch keine Bewertungen
- The Predictive Value of Malnutrition For Functional and Cognitive Status in Elderly Hemodialysis PatientsDokument8 SeitenThe Predictive Value of Malnutrition For Functional and Cognitive Status in Elderly Hemodialysis PatientsyafanitaizzatiNoch keine Bewertungen
- Association Between Anxiety and DepressionDokument10 SeitenAssociation Between Anxiety and Depressionoliffasalma atthahirohNoch keine Bewertungen
- Kead 348Dokument9 SeitenKead 348Alberto Sifuentes GiraldoNoch keine Bewertungen
- Jurnal Internasional Korea DMDokument9 SeitenJurnal Internasional Korea DMzahradeswitamuftiNoch keine Bewertungen
- The Impact of Malnutritional Status On Survival in Elderly Hemodialysis PatientsDokument5 SeitenThe Impact of Malnutritional Status On Survival in Elderly Hemodialysis PatientsTika MahelsaNoch keine Bewertungen
- 10Dokument6 Seiten10cicelynara94Noch keine Bewertungen
- Prevalence, Risk Factors, Adherence and Non Adherence in Patient With Chronic Kidney Disease: A Prospective StudyDokument7 SeitenPrevalence, Risk Factors, Adherence and Non Adherence in Patient With Chronic Kidney Disease: A Prospective StudyRanitaRahmaniarNoch keine Bewertungen
- An Observational Study of Effect On Lipid Profile by Short Term Use of Low Dose Steroid Therapy in Common Orthopaedic ConditionsDokument7 SeitenAn Observational Study of Effect On Lipid Profile by Short Term Use of Low Dose Steroid Therapy in Common Orthopaedic ConditionsIJAR JOURNALNoch keine Bewertungen
- Factors Predicting Malnutrition in Hemodialysis Patients: A Cross-Sectional StudyDokument10 SeitenFactors Predicting Malnutrition in Hemodialysis Patients: A Cross-Sectional StudyMarco TolentinoNoch keine Bewertungen
- EJMCM - Volume 10 - Issue 4 - Pages 893-903Dokument11 SeitenEJMCM - Volume 10 - Issue 4 - Pages 893-903Junaid IwqNoch keine Bewertungen
- Obese Viser AlDokument7 SeitenObese Viser AlIzzatul MaghfirohNoch keine Bewertungen
- GoutDokument17 SeitenGoutnadita erischaNoch keine Bewertungen
- (2019) - Breakfast Association With Arterial Stiffness and Carotid Atherosclerotic Burden. Insights From The Corinthia Study. Nutrition, MetabolDokument7 Seiten(2019) - Breakfast Association With Arterial Stiffness and Carotid Atherosclerotic Burden. Insights From The Corinthia Study. Nutrition, MetabolMaria RamonaNoch keine Bewertungen
- Diagnostico de La EDDokument6 SeitenDiagnostico de La EDJuan Sebastian Quintero BoteroNoch keine Bewertungen
- 1 s2.0 S1871402120304069 MainDokument9 Seiten1 s2.0 S1871402120304069 MainChiranjeeviNoch keine Bewertungen
- Impact of Pharmaceutical Care On The Health-RelateDokument14 SeitenImpact of Pharmaceutical Care On The Health-RelatealfinadyaNoch keine Bewertungen
- J of Gastro and Hepatol - 2021 - Kim - Association Between Metabolic Syndrome and Incidence of Cholelithiasis in The KoreanDokument8 SeitenJ of Gastro and Hepatol - 2021 - Kim - Association Between Metabolic Syndrome and Incidence of Cholelithiasis in The Koreanrahmat akbarNoch keine Bewertungen
- JurnalDokument8 SeitenJurnalQinthara MuftiNoch keine Bewertungen
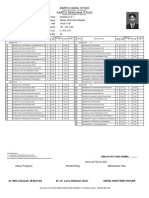
- Kartu Hasil Studi Kartu Rencana StudiDokument2 SeitenKartu Hasil Studi Kartu Rencana StudiQinthara MuftiNoch keine Bewertungen
- How Does Obesity Affect The Endocrine System - A Narrative ReviewDokument9 SeitenHow Does Obesity Affect The Endocrine System - A Narrative ReviewQinthara MuftiNoch keine Bewertungen
- Association Between Pregnancy and Perinatal Outcomes Among Women With EpilepsyDokument9 SeitenAssociation Between Pregnancy and Perinatal Outcomes Among Women With EpilepsyQinthara MuftiNoch keine Bewertungen
- Pembimbing Tugas Koas Bedah RSUP Persahabatan Periode 26 Agustus S.D. 2 November 2019Dokument2 SeitenPembimbing Tugas Koas Bedah RSUP Persahabatan Periode 26 Agustus S.D. 2 November 2019Qinthara MuftiNoch keine Bewertungen
- DafpusDokument3 SeitenDafpusQinthara MuftiNoch keine Bewertungen
- Daftar PustakaDokument9 SeitenDaftar PustakaQinthara MuftiNoch keine Bewertungen
- "What Are The Effects of Moderate Drinking On Stroke Risk?": Continuing Medical EducationDokument13 Seiten"What Are The Effects of Moderate Drinking On Stroke Risk?": Continuing Medical EducationQinthara MuftiNoch keine Bewertungen
- Pembimbing Tugas Koas Bedah RSUP Persahabatan Periode 26 Agustus S.D. 2 November 2019Dokument2 SeitenPembimbing Tugas Koas Bedah RSUP Persahabatan Periode 26 Agustus S.D. 2 November 2019Qinthara MuftiNoch keine Bewertungen
- Rekapitulasi Nilai PretestDokument1 SeiteRekapitulasi Nilai PretestQinthara MuftiNoch keine Bewertungen
- OUTPUTDokument1 SeiteOUTPUTQinthara MuftiNoch keine Bewertungen
- Management of Pterygium: DR Vidyashankar G K Shekar Nethralaya BangaloreDokument18 SeitenManagement of Pterygium: DR Vidyashankar G K Shekar Nethralaya BangaloreelisgretyNoch keine Bewertungen
- Tanya Catering ServiceDokument6 SeitenTanya Catering ServiceQinthara MuftiNoch keine Bewertungen
- Tatalaksana HypoparathyroidismDokument13 SeitenTatalaksana HypoparathyroidismQinthara MuftiNoch keine Bewertungen
- OutputDokument1 SeiteOutputEthan NguyễnNoch keine Bewertungen
- Play ClawDokument2 SeitenPlay ClawFrenda SeivelunNoch keine Bewertungen
- Electrical Engineering Lab Vica AnDokument6 SeitenElectrical Engineering Lab Vica Anabdulnaveed50% (2)
- DCN Dte-Dce and ModemsDokument5 SeitenDCN Dte-Dce and ModemsSathish BabuNoch keine Bewertungen
- Literature Review of Service Quality in RestaurantsDokument7 SeitenLiterature Review of Service Quality in RestaurantsuifjzvrifNoch keine Bewertungen
- UAV Design TrainingDokument17 SeitenUAV Design TrainingPritam AshutoshNoch keine Bewertungen
- Oceanarium: Welcome To The Museum Press ReleaseDokument2 SeitenOceanarium: Welcome To The Museum Press ReleaseCandlewick PressNoch keine Bewertungen
- Impact of Government Policies and EthicsDokument24 SeitenImpact of Government Policies and EthicsGunveen AbrolNoch keine Bewertungen
- Directorate of Technical Education, Admission Committee For Professional Courses (ACPC), GujaratDokument2 SeitenDirectorate of Technical Education, Admission Committee For Professional Courses (ACPC), GujaratgamailkabaaaapNoch keine Bewertungen
- 105 2Dokument17 Seiten105 2Diego TobrNoch keine Bewertungen
- Web-Based Attendance Management System Using Bimodal Authentication TechniquesDokument61 SeitenWeb-Based Attendance Management System Using Bimodal Authentication TechniquesajextopeNoch keine Bewertungen
- Motivation Theories Description and CriticismDokument14 SeitenMotivation Theories Description and CriticismAhmed Elgazzar89% (18)
- G1000 Us 1014 PDFDokument820 SeitenG1000 Us 1014 PDFLuís Miguel RomãoNoch keine Bewertungen
- Community Architecture Concept PDFDokument11 SeitenCommunity Architecture Concept PDFdeanNoch keine Bewertungen
- Past Simple Vs Past ContinuousDokument3 SeitenPast Simple Vs Past ContinuousNatalia SalinasNoch keine Bewertungen
- Latest ResumeDokument2 SeitenLatest Resumesamy1234567Noch keine Bewertungen
- Verniers Micrometers and Measurement Uncertainty and Digital2Dokument30 SeitenVerniers Micrometers and Measurement Uncertainty and Digital2Raymond ScottNoch keine Bewertungen
- Procter and Gamble - MarketingDokument10 SeitenProcter and Gamble - MarketingIvana Panovska100% (5)
- STS Module 11Dokument64 SeitenSTS Module 11Desiree GalletoNoch keine Bewertungen
- IMDSI22Dokument82 SeitenIMDSI22Dang JinlongNoch keine Bewertungen
- Coal Bottom Ash As Sand Replacement in ConcreteDokument9 SeitenCoal Bottom Ash As Sand Replacement in ConcretexxqNoch keine Bewertungen
- E-Mobility and SafetyDokument77 SeitenE-Mobility and SafetySantosh KumarNoch keine Bewertungen
- Vieworks DR Panel BrochureDokument8 SeitenVieworks DR Panel Brochuretito goodNoch keine Bewertungen
- Clint Freeman ResumeDokument2 SeitenClint Freeman ResumeClint Tiberius FreemanNoch keine Bewertungen
- Preparing For CPHQ .. An Overview of Concepts: Ghada Al-BarakatiDokument109 SeitenPreparing For CPHQ .. An Overview of Concepts: Ghada Al-BarakatiBilal SalamehNoch keine Bewertungen
- Sainik School Balachadi: Name-Class - Roll No - Subject - House - Assigned byDokument10 SeitenSainik School Balachadi: Name-Class - Roll No - Subject - House - Assigned byPagalNoch keine Bewertungen
- Additional Article Information: Keywords: Adenoid Cystic Carcinoma, Cribriform Pattern, Parotid GlandDokument7 SeitenAdditional Article Information: Keywords: Adenoid Cystic Carcinoma, Cribriform Pattern, Parotid GlandRizal TabootiNoch keine Bewertungen
- Enrile v. SalazarDokument26 SeitenEnrile v. SalazarMaria Aerial AbawagNoch keine Bewertungen
- Digital Electronics Chapter 5Dokument30 SeitenDigital Electronics Chapter 5Pious TraderNoch keine Bewertungen
- Advertisement: National Institute of Technology, Tiruchirappalli - 620 015 TEL: 0431 - 2503365, FAX: 0431 - 2500133Dokument4 SeitenAdvertisement: National Institute of Technology, Tiruchirappalli - 620 015 TEL: 0431 - 2503365, FAX: 0431 - 2500133dineshNoch keine Bewertungen
- Strategic Marketing: The University of Lahore (Islamabad Campus)Dokument3 SeitenStrategic Marketing: The University of Lahore (Islamabad Campus)Sumaira IrshadNoch keine Bewertungen
- The Obesity Code: Unlocking the Secrets of Weight LossVon EverandThe Obesity Code: Unlocking the Secrets of Weight LossBewertung: 4 von 5 Sternen4/5 (6)
- By the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsVon EverandBy the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsNoch keine Bewertungen
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeVon EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeBewertung: 2 von 5 Sternen2/5 (1)
- The Age of Magical Overthinking: Notes on Modern IrrationalityVon EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityBewertung: 4 von 5 Sternen4/5 (24)
- The Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaVon EverandThe Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- Summary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisVon EverandSummary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisBewertung: 4.5 von 5 Sternen4.5/5 (42)
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedVon EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedBewertung: 5 von 5 Sternen5/5 (80)
- ADHD is Awesome: A Guide to (Mostly) Thriving with ADHDVon EverandADHD is Awesome: A Guide to (Mostly) Thriving with ADHDBewertung: 5 von 5 Sternen5/5 (1)
- Self-Care for Autistic People: 100+ Ways to Recharge, De-Stress, and Unmask!Von EverandSelf-Care for Autistic People: 100+ Ways to Recharge, De-Stress, and Unmask!Bewertung: 5 von 5 Sternen5/5 (1)
- Raising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsVon EverandRaising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsBewertung: 5 von 5 Sternen5/5 (1)
- Outlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisVon EverandOutlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisBewertung: 4 von 5 Sternen4/5 (1)
- The Comfort of Crows: A Backyard YearVon EverandThe Comfort of Crows: A Backyard YearBewertung: 4.5 von 5 Sternen4.5/5 (23)
- Dark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Von EverandDark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Bewertung: 4.5 von 5 Sternen4.5/5 (110)
- Gut: the new and revised Sunday Times bestsellerVon EverandGut: the new and revised Sunday Times bestsellerBewertung: 4 von 5 Sternen4/5 (392)
- Why We Die: The New Science of Aging and the Quest for ImmortalityVon EverandWhy We Die: The New Science of Aging and the Quest for ImmortalityBewertung: 4 von 5 Sternen4/5 (3)
- Raising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsVon EverandRaising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsBewertung: 4.5 von 5 Sternen4.5/5 (169)
- Cult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryVon EverandCult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryBewertung: 4 von 5 Sternen4/5 (44)
- Mindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessVon EverandMindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessBewertung: 4.5 von 5 Sternen4.5/5 (328)
- The Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsVon EverandThe Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsBewertung: 3.5 von 5 Sternen3.5/5 (3)
- When the Body Says No by Gabor Maté: Key Takeaways, Summary & AnalysisVon EverandWhen the Body Says No by Gabor Maté: Key Takeaways, Summary & AnalysisBewertung: 3.5 von 5 Sternen3.5/5 (2)
- Sleep Stories for Adults: Overcome Insomnia and Find a Peaceful AwakeningVon EverandSleep Stories for Adults: Overcome Insomnia and Find a Peaceful AwakeningBewertung: 4 von 5 Sternen4/5 (3)
- Gut: The Inside Story of Our Body's Most Underrated Organ (Revised Edition)Von EverandGut: The Inside Story of Our Body's Most Underrated Organ (Revised Edition)Bewertung: 4 von 5 Sternen4/5 (378)
- To Explain the World: The Discovery of Modern ScienceVon EverandTo Explain the World: The Discovery of Modern ScienceBewertung: 3.5 von 5 Sternen3.5/5 (51)
- The Marshmallow Test: Mastering Self-ControlVon EverandThe Marshmallow Test: Mastering Self-ControlBewertung: 4.5 von 5 Sternen4.5/5 (58)