Das könnte Ihnen auch gefallen
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (121)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (400)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2259)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
- EFFECTS OF Emotional AbuseDokument13 SeitenEFFECTS OF Emotional AbuseJoshua Tardiff100% (1)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (74)
- Trauma Presentation WebsiteDokument19 SeitenTrauma Presentation Websiteapi-559672171Noch keine Bewertungen
- Effective Team Leadership 2008 PDFDokument71 SeitenEffective Team Leadership 2008 PDFshekhar083100% (1)
- Role of Attitude in Multicultural Counseling - Minami (2009)Dokument8 SeitenRole of Attitude in Multicultural Counseling - Minami (2009)xiejie22590Noch keine Bewertungen
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- How Are IQ and EQ Measured and TestedDokument3 SeitenHow Are IQ and EQ Measured and TestedRodel YapNoch keine Bewertungen
- BCJ582 Final Exam 100% Correct AnswersDokument49 SeitenBCJ582 Final Exam 100% Correct AnswersHomeworkhelpbylance0% (3)
- Training Attendance Sheet & Feedback FormDokument6 SeitenTraining Attendance Sheet & Feedback FormAmaresh NayakNoch keine Bewertungen
- A Beautiful Mind MSEDokument10 SeitenA Beautiful Mind MSECarla Rosyl Fuentes100% (3)
- Mock Job Interview Question and Rating SheetDokument1 SeiteMock Job Interview Question and Rating SheetVictoria Quebral CarumbaNoch keine Bewertungen
- Outpatient Continued Stay Review 6316Dokument2 SeitenOutpatient Continued Stay Review 6316Mistor Dupois WilliamsNoch keine Bewertungen
- 4Dokument31 Seiten4CzarinaTagbakNoch keine Bewertungen
- SHDP Application Project Concept Note Template v. 1.1.22january2016Dokument3 SeitenSHDP Application Project Concept Note Template v. 1.1.22january2016Joldan Lambino100% (1)
- Roles of Educational Technology in LearningDokument39 SeitenRoles of Educational Technology in LearningNhazkie Block100% (2)
- Lo 3Dokument1 SeiteLo 3Cbr 150Noch keine Bewertungen
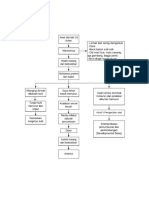
- Mind Mapping MarasmusDokument1 SeiteMind Mapping MarasmusCbr 150Noch keine Bewertungen
- Karakteristik Ulkus Diabetikum Pada Penderita Diabetes Mellitus Di RSUD Dr. Zainal Abidin Dan RSUD Meuraxa Banda AcehDokument8 SeitenKarakteristik Ulkus Diabetikum Pada Penderita Diabetes Mellitus Di RSUD Dr. Zainal Abidin Dan RSUD Meuraxa Banda AcehSabriNoch keine Bewertungen
- 1215 2513 1 SM PDFDokument13 Seiten1215 2513 1 SM PDFtary_nuryanaNoch keine Bewertungen
- Stress Management and Employee Productivity An Examination of The Nigerian Work EnvironmentDokument8 SeitenStress Management and Employee Productivity An Examination of The Nigerian Work EnvironmentInternational Journal of Innovative Science and Research TechnologyNoch keine Bewertungen
- Different Sources of Stress Among Grade 11 Stem Students of San Juan de Dios Educational Foundation Inc. - College On First Semester Academic Year 2018 - 2019Dokument7 SeitenDifferent Sources of Stress Among Grade 11 Stem Students of San Juan de Dios Educational Foundation Inc. - College On First Semester Academic Year 2018 - 2019Janne KyutNoch keine Bewertungen
- PA y Depresión en Nepal 2017Dokument8 SeitenPA y Depresión en Nepal 2017Alfredo PérezNoch keine Bewertungen
- Assignment 2 Elt 200Dokument2 SeitenAssignment 2 Elt 200Vanessa S. MoludNoch keine Bewertungen
- Classroom Management-The TeacherDokument21 SeitenClassroom Management-The TeacherPatricia María Guillén Cuamatzi100% (1)
- Resea RRR CHDokument4 SeitenResea RRR CHimsana minatozakiNoch keine Bewertungen
- ISTE National Educational Technology Standards For Students (NETSFS)Dokument23 SeitenISTE National Educational Technology Standards For Students (NETSFS)Shairon palmaNoch keine Bewertungen
- Universal Design For Learning (UDL) Lesson Plan Evaluation and RedesignDokument4 SeitenUniversal Design For Learning (UDL) Lesson Plan Evaluation and Redesignapi-458501224Noch keine Bewertungen
- Logic 2Dokument2 SeitenLogic 2augustine abellanaNoch keine Bewertungen
- What Is Explicit InstructionDokument9 SeitenWhat Is Explicit InstructionMelba L. AlipustainNoch keine Bewertungen
- Teacher InterviewDokument4 SeitenTeacher Interviewapi-241849160Noch keine Bewertungen
- Manual de Aplicación MapiDokument7 SeitenManual de Aplicación MapiEmily ChurunelNoch keine Bewertungen
- Field Experience Reflection EssayDokument2 SeitenField Experience Reflection EssayRainer Arthur LarocoNoch keine Bewertungen
- Quality of Work LifeDokument10 SeitenQuality of Work LifeAzula AzulaNoch keine Bewertungen
- Year 3 Civic Lesson Plan (January-Love) : By:MissashDokument1 SeiteYear 3 Civic Lesson Plan (January-Love) : By:MissashJason Fleming0% (1)
- IGNOU CERTIFICATE IN TEACHING OF ENGLISH CTE-3 - Jun - 2017 Question PaperDokument3 SeitenIGNOU CERTIFICATE IN TEACHING OF ENGLISH CTE-3 - Jun - 2017 Question PaperTelika RamuNoch keine Bewertungen
- The Effects of Organizational Citizenship Behavior On Performance Judgments: A Field Study and A Laboratory ExperimentDokument14 SeitenThe Effects of Organizational Citizenship Behavior On Performance Judgments: A Field Study and A Laboratory ExperimentNofri Adita HopeNoch keine Bewertungen