Das könnte Ihnen auch gefallen
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (345)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (121)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (74)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- EMRA EMS EssentialsDokument167 SeitenEMRA EMS EssentialsMiko Ramoso100% (3)
- Disseminated Intravascular Coagulation - Background, Pathophysiology, EtiologyDokument11 SeitenDisseminated Intravascular Coagulation - Background, Pathophysiology, Etiologyevi100% (2)
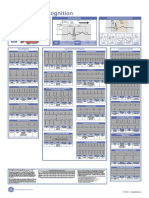
- Poster1 Arrhythmia Recognition e PDFDokument1 SeitePoster1 Arrhythmia Recognition e PDFMiko RamosoNoch keine Bewertungen
- ECGcheatsheet5 PDFDokument1 SeiteECGcheatsheet5 PDFMiko Ramoso100% (1)
- Legal MedicineDokument2 SeitenLegal MedicineMiko RamosoNoch keine Bewertungen
- ArvindbhaiDokument1 SeiteArvindbhaiJ D PatelNoch keine Bewertungen
- Policy and Procedure Infection Control FinalDokument226 SeitenPolicy and Procedure Infection Control FinalWandy SejeliNoch keine Bewertungen
- Zoonotic DiseasesDokument27 SeitenZoonotic DiseasesGift Summer DinoNoch keine Bewertungen
- Epidemiology Lectures by Dr. MabalatanDokument8 SeitenEpidemiology Lectures by Dr. MabalatanCitrusNoch keine Bewertungen
- Worm Infestation in ChildrenDokument4 SeitenWorm Infestation in ChildrenOleOhhNoch keine Bewertungen
- Colposcopy, Cervical Screening, and HPV, An Issue of Obstetrics and Gynecology Clinics (The Clinics - Internal Medicine)Dokument155 SeitenColposcopy, Cervical Screening, and HPV, An Issue of Obstetrics and Gynecology Clinics (The Clinics - Internal Medicine)Annca RoXanna100% (1)
- PRELIM Third Periodical Test in MAPEHDokument3 SeitenPRELIM Third Periodical Test in MAPEHAnne Santos RojoNoch keine Bewertungen
- Sepsis Guidelines 2012Dokument13 SeitenSepsis Guidelines 2012Lauren WilkersonNoch keine Bewertungen
- P. Malariae P. Vivax P. Ovale P. Falciparum P. Knowlesi: PlasmodiaDokument6 SeitenP. Malariae P. Vivax P. Ovale P. Falciparum P. Knowlesi: PlasmodiaJustin TayabanNoch keine Bewertungen
- ICU Guide OneDokument318 SeitenICU Guide OneSamar DakkakNoch keine Bewertungen
- Experiment #5 - Isolation of Normal FloraDokument9 SeitenExperiment #5 - Isolation of Normal FloraFrancis MagbitangNoch keine Bewertungen
- 1.2 Nucleic Acids, Biology For Engineers DRPDokument4 Seiten1.2 Nucleic Acids, Biology For Engineers DRPShreya shresthNoch keine Bewertungen
- 2014 CCM Review Notes Jon-Emile S. Kenny M.D, 2014Dokument142 Seiten2014 CCM Review Notes Jon-Emile S. Kenny M.D, 2014PkernNoch keine Bewertungen
- Aspergillosis IDSA GuidelinesDokument34 SeitenAspergillosis IDSA GuidelinesAndreas IoannouNoch keine Bewertungen
- Source Information: Disclosure FormsDokument1 SeiteSource Information: Disclosure FormsSav GaNoch keine Bewertungen
- SPM MeaslesDokument30 SeitenSPM MeaslesAri YudiNoch keine Bewertungen
- Dengue CPDokument26 SeitenDengue CPChinchu MohanNoch keine Bewertungen
- Viruses and Bacteria BingoDokument3 SeitenViruses and Bacteria Bingoapi-252119803Noch keine Bewertungen
- Poultry McqsDokument3 SeitenPoultry McqsWaqas NawazNoch keine Bewertungen
- Antifungal DrugsDokument20 SeitenAntifungal DrugsboeykhNoch keine Bewertungen
- A Diagnostic Approach To PruritusDokument8 SeitenA Diagnostic Approach To PruritusSpica AdharaNoch keine Bewertungen
- Benign WBC Disorders Third YaerDokument27 SeitenBenign WBC Disorders Third YaerAisho KeyfNoch keine Bewertungen
- Biology Complete Important Mcqs For Medical Entry Test PreparationDokument24 SeitenBiology Complete Important Mcqs For Medical Entry Test PreparationaamirNoch keine Bewertungen
- (EPI) 1.01 - Overview of Epidemiology & Descriptive Epidemiology - Dr. ButacanDokument5 Seiten(EPI) 1.01 - Overview of Epidemiology & Descriptive Epidemiology - Dr. Butacanpasambalyrradjohndar0% (1)
- Formal Letter - Poor Conditions in Housing EstateDokument2 SeitenFormal Letter - Poor Conditions in Housing EstateJessica Kong50% (2)
- National Tuberculosis Control ProgramDokument3 SeitenNational Tuberculosis Control ProgrampeterjongNoch keine Bewertungen
- MC 0628Dokument20 SeitenMC 0628mcchronicleNoch keine Bewertungen
- Med AtbDokument3 SeitenMed AtbพัชรพลนะเออNoch keine Bewertungen
- Skin Donation Information GuideDokument2 SeitenSkin Donation Information GuidedrnikhilpanseNoch keine Bewertungen