Das könnte Ihnen auch gefallen
- 11 Recurrent Aphthous Stomatitis Caused by Food AllergyDokument6 Seiten11 Recurrent Aphthous Stomatitis Caused by Food AllergyramaNoch keine Bewertungen
- 1 PB PDFDokument6 Seiten1 PB PDFramaNoch keine Bewertungen
- Gingival Pigmentation and Its Treatment ModalititesDokument4 SeitenGingival Pigmentation and Its Treatment ModalititesramaNoch keine Bewertungen
- Depigmentation of Gingiva PDFDokument3 SeitenDepigmentation of Gingiva PDFramaNoch keine Bewertungen
- 2007 - Exfoliative Cheilitis A Case ReportDokument5 Seiten2007 - Exfoliative Cheilitis A Case ReportramaNoch keine Bewertungen
- Reference Sinus Lifting Untuk Pemasangan Implan Pada Rahang AtasDokument5 SeitenReference Sinus Lifting Untuk Pemasangan Implan Pada Rahang AtasramaNoch keine Bewertungen
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (400)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (74)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (345)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (121)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- 0003-3219 (2002) 0720387-Eovtfd2 0 Co 2Dokument10 Seiten0003-3219 (2002) 0720387-Eovtfd2 0 Co 2Cesar Ivan Lopez MtzNoch keine Bewertungen
- Normal Anatomy of RadiologyDokument44 SeitenNormal Anatomy of RadiologySelvaraj ChinnasamyNoch keine Bewertungen
- Morphology of Primary Dentition PPT 1Dokument29 SeitenMorphology of Primary Dentition PPT 1Santhoshi ReddyNoch keine Bewertungen
- 1 SM PDFDokument3 Seiten1 SM PDFNurul NoviasariNoch keine Bewertungen
- Anatomical Landmarks of The CrownDokument3 SeitenAnatomical Landmarks of The CrownHayley WelshNoch keine Bewertungen
- A Clinical Guide To Occlusion An IntroductionDokument75 SeitenA Clinical Guide To Occlusion An IntroductionAndrei Oana100% (1)
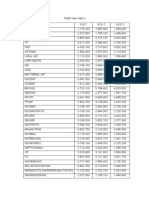
- Tarif Ina CBGDokument2 SeitenTarif Ina CBGoctavia tri wulandariNoch keine Bewertungen
- Presented By:-Samson S. Samuel 1 Year Guided By: - Dr. Fatima Saify Dr. Nidhi Sharma Dr. Kedarnath AgarwalDokument20 SeitenPresented By:-Samson S. Samuel 1 Year Guided By: - Dr. Fatima Saify Dr. Nidhi Sharma Dr. Kedarnath AgarwalDrBhawna AroraNoch keine Bewertungen
- Reasons For Extraction of Primary Teeth in Jordan-A Study.: August 2013Dokument5 SeitenReasons For Extraction of Primary Teeth in Jordan-A Study.: August 2013Mutia KumalasariNoch keine Bewertungen
- Intra Oral Periapical Radiography - Basics Yet Intrigue: A ReviewDokument6 SeitenIntra Oral Periapical Radiography - Basics Yet Intrigue: A ReviewsalsaNoch keine Bewertungen
- Ipdoaj MS Id 000113Dokument3 SeitenIpdoaj MS Id 000113Ayu DamayNoch keine Bewertungen
- CH 3 Partial Coverage RetainersDokument25 SeitenCH 3 Partial Coverage Retainerssolom islamNoch keine Bewertungen
- Development of ToothDokument68 SeitenDevelopment of Toothpvspartan0933% (3)
- Dimensional Changes of The Deciduos Dental Arch Class I With Crowding, Using Direct Planas Tracks. Medellin 2012-2013Dokument10 SeitenDimensional Changes of The Deciduos Dental Arch Class I With Crowding, Using Direct Planas Tracks. Medellin 2012-2013Miguel candelaNoch keine Bewertungen
- Teeth: Miss Sandy TseDokument21 SeitenTeeth: Miss Sandy Tseyin_sandy1129Noch keine Bewertungen
- Andrews 6 Keys of Normal OcclusionDokument2 SeitenAndrews 6 Keys of Normal OcclusionKaren AlfredNoch keine Bewertungen
- Complications in Endodontic SurgeryDokument198 SeitenComplications in Endodontic SurgeryASDASDADSDNoch keine Bewertungen
- Pendahuluan Mastikasi: Suatu Pola TetapDokument28 SeitenPendahuluan Mastikasi: Suatu Pola TetapBirgitaCaresaNoch keine Bewertungen
- Mandibular IncisorsDokument13 SeitenMandibular IncisorsVishal PatelNoch keine Bewertungen
- Section - 035 - Denture Occlusion OverviewDokument3 SeitenSection - 035 - Denture Occlusion OverviewAravind KrishnanNoch keine Bewertungen
- Single Tooth Bite Forces in Healthy Young Adults: V.F.Ferrario, C.Sforza, G.Serrao, C.Dellavia&G.M.TartagliaDokument5 SeitenSingle Tooth Bite Forces in Healthy Young Adults: V.F.Ferrario, C.Sforza, G.Serrao, C.Dellavia&G.M.TartagliaChloeee GNoch keine Bewertungen
- Selective Grinding in Complete DentureDokument10 SeitenSelective Grinding in Complete Denturevarun100% (1)
- Ortho Lecture 1Dokument4 SeitenOrtho Lecture 1api-101745006Noch keine Bewertungen
- Diagnosis and Treatment Planning in FPDDokument46 SeitenDiagnosis and Treatment Planning in FPDSujanaNoch keine Bewertungen
- Cast Gold Crown PreparationDokument24 SeitenCast Gold Crown PreparationDenisse MacNoch keine Bewertungen
- Mock 4 DR.M PDFDokument18 SeitenMock 4 DR.M PDFHarjotBrarNoch keine Bewertungen
- Department of OrthodonticsDokument23 SeitenDepartment of OrthodonticsDevilish EggsNoch keine Bewertungen
- Altered Passive Eruption and Active Secondary EruptionDokument25 SeitenAltered Passive Eruption and Active Secondary EruptionBenjiNoch keine Bewertungen
- Republic of The Philippine4 OrthodonticsDokument84 SeitenRepublic of The Philippine4 OrthodonticsGo IdeasNoch keine Bewertungen
- 5.permanent Mandibular First MolarDokument13 Seiten5.permanent Mandibular First Molardr-ahmedyu100% (1)