Das könnte Ihnen auch gefallen
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (119)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (399)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (587)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2219)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (344)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (890)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (73)
- Research10 q3 Mod2 InterpretationofData v3Dokument24 SeitenResearch10 q3 Mod2 InterpretationofData v3Dalissa Rivadeniera0% (3)
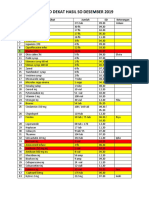
- Daftar Stok Ruang Alkes VKDokument1 SeiteDaftar Stok Ruang Alkes VKCitra DewiNoch keine Bewertungen
- Stok Ruangan IgdDokument11 SeitenStok Ruangan IgdCitra DewiNoch keine Bewertungen
- Caviplex multivitamin documentDokument20 SeitenCaviplex multivitamin documentCitra DewiNoch keine Bewertungen
- RS SIDOWARAS Pengajuan Anggaran Obat & Alkes (Kredit) 14 Januari 2019Dokument323 SeitenRS SIDOWARAS Pengajuan Anggaran Obat & Alkes (Kredit) 14 Januari 2019Citra DewiNoch keine Bewertungen
- SurgicalDokument44 SeitenSurgicalgisellapramuditaNoch keine Bewertungen
- 37 423 1 SPDokument8 Seiten37 423 1 SPBelladonna Perdana PutraNoch keine Bewertungen
- DDD Februari 2018Dokument12 SeitenDDD Februari 2018Citra DewiNoch keine Bewertungen
- KamuDokument2 SeitenKamuCitra DewiNoch keine Bewertungen
- List of Farmacy Graduates with Gender and ReligionDokument30 SeitenList of Farmacy Graduates with Gender and ReligionCitra DewiNoch keine Bewertungen
- ANADIUM MEDIAMER ARTRODAR CHLOROQUIN MEDICATION LIST LESS THAN 40 CHARACTERSDokument24 SeitenANADIUM MEDIAMER ARTRODAR CHLOROQUIN MEDICATION LIST LESS THAN 40 CHARACTERSCitra DewiNoch keine Bewertungen
- List of Farmacy Graduates with Gender and ReligionDokument30 SeitenList of Farmacy Graduates with Gender and ReligionCitra DewiNoch keine Bewertungen
- KamuDokument2 SeitenKamuCitra DewiNoch keine Bewertungen
- 37 423 1 SPDokument8 Seiten37 423 1 SPBelladonna Perdana PutraNoch keine Bewertungen
- Bahan Habis Pakai Operasi PakdirDokument701 SeitenBahan Habis Pakai Operasi PakdirCitra DewiNoch keine Bewertungen
- Paket Alkes Per SpesialisDokument58 SeitenPaket Alkes Per SpesialisCitra DewiNoch keine Bewertungen
- PupDokument21 SeitenPupCitra DewiNoch keine Bewertungen
- Calcium Lactate Anhydrous PDFDokument6 SeitenCalcium Lactate Anhydrous PDFCitra DewiNoch keine Bewertungen
- Bahan Habis Pakai Operasi PakdirDokument701 SeitenBahan Habis Pakai Operasi PakdirCitra DewiNoch keine Bewertungen
- CV CreatewinningcvDokument11 SeitenCV CreatewinningcvshrirangkattiNoch keine Bewertungen
- CV CreatewinningcvDokument11 SeitenCV CreatewinningcvshrirangkattiNoch keine Bewertungen
- CV Examples: How to Highlight Skills & AchievementsDokument8 SeitenCV Examples: How to Highlight Skills & AchievementsCrye BiggieNoch keine Bewertungen
- Emulsion IpcDokument12 SeitenEmulsion IpcCitra DewiNoch keine Bewertungen
- Calcium Lactate1Dokument2 SeitenCalcium Lactate1Citra DewiNoch keine Bewertungen
- Department of Health and Human Services: Vol. 79 Thursday, No. 233 December 4, 2014Dokument41 SeitenDepartment of Health and Human Services: Vol. 79 Thursday, No. 233 December 4, 2014Citra DewiNoch keine Bewertungen
- Surabaya, 2017 Dosen Pembimbing Preseptor: Kode OutcomeDokument1 SeiteSurabaya, 2017 Dosen Pembimbing Preseptor: Kode OutcomeCitra DewiNoch keine Bewertungen
- Walkability Surveys in Asian Cities PDFDokument20 SeitenWalkability Surveys in Asian Cities PDFJason VillaNoch keine Bewertungen
- Science Process Skills Inventory (SPSI) : Oregon State University 4-H Youth DevelopmentDokument2 SeitenScience Process Skills Inventory (SPSI) : Oregon State University 4-H Youth DevelopmentTessie Rose ColasNoch keine Bewertungen
- Philippine Seven PESTEL AnalysisDokument2 SeitenPhilippine Seven PESTEL AnalysisLyanna MormontNoch keine Bewertungen
- Review of LiteratureDokument78 SeitenReview of Literaturesm_bolke_422802317Noch keine Bewertungen
- Hoy C6 LeadershipDokument23 SeitenHoy C6 LeadershipMohd Hafiz JasmiNoch keine Bewertungen
- The 42 V's of Big Data and Data Science PDFDokument6 SeitenThe 42 V's of Big Data and Data Science PDF5oscilantesNoch keine Bewertungen
- JD SR Sap MM Consultant PDFDokument2 SeitenJD SR Sap MM Consultant PDFSrinivas DsNoch keine Bewertungen
- Module 1 - Introduction To Managerial EconomicsDokument18 SeitenModule 1 - Introduction To Managerial EconomicsAmeen MahmoodNoch keine Bewertungen
- Research Paper SMPDokument5 SeitenResearch Paper SMPDevashishGuptaNoch keine Bewertungen
- Asthma Quality of Life PDFDokument102 SeitenAsthma Quality of Life PDFLuqmanul HakimNoch keine Bewertungen
- DCHB Town Release 0500 UkDokument214 SeitenDCHB Town Release 0500 Ukchan chadoNoch keine Bewertungen
- Herding Behaviour in The Chinese and Indian Stock Markets: Paulo Lao and Harminder SinghDokument31 SeitenHerding Behaviour in The Chinese and Indian Stock Markets: Paulo Lao and Harminder SinghLata KaushikNoch keine Bewertungen
- II PU STATISTICSudupiDokument4 SeitenII PU STATISTICSudupiCommunity Institute of Management StudiesNoch keine Bewertungen
- Growth Promotion Test Guide For Media Used in Sterility TestsDokument5 SeitenGrowth Promotion Test Guide For Media Used in Sterility Testshoria96Noch keine Bewertungen
- Machine Learning Mining CompaniesDokument5 SeitenMachine Learning Mining CompaniesCristian Sardón rojasNoch keine Bewertungen
- Development of Knowledge Base of Concrete Bridge Maintenance Syst PDFDokument109 SeitenDevelopment of Knowledge Base of Concrete Bridge Maintenance Syst PDFKristi LawrenceNoch keine Bewertungen
- Pitt-Rivers The Spanish Bull-FightDokument6 SeitenPitt-Rivers The Spanish Bull-FightHéctor MedinaNoch keine Bewertungen
- Performance Based Design of Buildings & Bridges For Enhanced Seismic ResilienceDokument8 SeitenPerformance Based Design of Buildings & Bridges For Enhanced Seismic ResilienceMohit JainNoch keine Bewertungen
- Recognizing Fake News Now A Required Subject in California Schools - Santa Cruz SentinelDokument4 SeitenRecognizing Fake News Now A Required Subject in California Schools - Santa Cruz SentineljekalopeNoch keine Bewertungen
- Chapter 1Dokument46 SeitenChapter 1Carl Angel BasaNoch keine Bewertungen
- Soil Resistivity Measurement and Interpretation Technique: Dr. Mahadev Unde, Vishal TatheDokument6 SeitenSoil Resistivity Measurement and Interpretation Technique: Dr. Mahadev Unde, Vishal TatheMilos BugarinovicNoch keine Bewertungen
- Statistics Mcqs Paper 2013Dokument2 SeitenStatistics Mcqs Paper 2013zeb4019100% (1)
- Liceo Grad Studies Thesis FrameworkDokument19 SeitenLiceo Grad Studies Thesis FrameworkVane UcatNoch keine Bewertungen
- Duke University Press Fall 2012 CatalogDokument52 SeitenDuke University Press Fall 2012 CatalogDuke University PressNoch keine Bewertungen
- Fish Scales and Cuttlebones As Tile ComponentDokument9 SeitenFish Scales and Cuttlebones As Tile ComponentRezlynNoch keine Bewertungen
- Participatory M&E in Development PracticeDokument11 SeitenParticipatory M&E in Development PracticeCamille Mangay-ayamNoch keine Bewertungen
- Armfield and Heaton - 2013 - Management of Fear and Anxiety in The Dental Clinic - A ReviewDokument18 SeitenArmfield and Heaton - 2013 - Management of Fear and Anxiety in The Dental Clinic - A ReviewdiegowildbergerNoch keine Bewertungen
- An Empirical Study On Audit Expectation Gap Role of Auditing Education in BangladeshDokument17 SeitenAn Empirical Study On Audit Expectation Gap Role of Auditing Education in Bangladeshrajeshaisdu009100% (1)
- OrDokument3 SeitenOrsatishsaga1990Noch keine Bewertungen