Das könnte Ihnen auch gefallen
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (400)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (345)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (74)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2259)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (121)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- Urine SedimentDokument38 SeitenUrine Sedimentcyrhenmie100% (1)
- How To Make Your Own Colloidal SilverDokument21 SeitenHow To Make Your Own Colloidal Silverrawzero92% (12)
- Pathology Mcqs 2Dokument6 SeitenPathology Mcqs 2Numan Rox100% (5)
- Benzene MSDSDokument12 SeitenBenzene MSDSTom Jose KooduthottiyilNoch keine Bewertungen
- Benefits of Green TeaDokument3 SeitenBenefits of Green TeaVickey Kumar DhingraNoch keine Bewertungen
- What Are Pituitary Tumors?Dokument43 SeitenWhat Are Pituitary Tumors?S GrayNoch keine Bewertungen
- Irfan Mir NotesDokument199 SeitenIrfan Mir NotesSwathi AnantulaNoch keine Bewertungen
- DD Palmer Forgotten TheoriesDokument10 SeitenDD Palmer Forgotten TheoriesSamNoch keine Bewertungen
- Thyroid Gland NotesDokument21 SeitenThyroid Gland NotesbryanNoch keine Bewertungen
- Esclerosis Lateral Amiotrofica (Ela) : TratamientoDokument2 SeitenEsclerosis Lateral Amiotrofica (Ela) : TratamientoMelissa Cruzado Valdivia100% (1)
- Plasma Cell Dyscrasia: Sri Kartika SariDokument35 SeitenPlasma Cell Dyscrasia: Sri Kartika SariSelimatul AlpaeniNoch keine Bewertungen
- TEST I - Foundation of Professional Nursing PracticeDokument11 SeitenTEST I - Foundation of Professional Nursing Practiceraquel maniegoNoch keine Bewertungen
- Laminate Safety Data SheetDokument4 SeitenLaminate Safety Data SheetNicasio AllonarNoch keine Bewertungen
- GTD TogDokument6 SeitenGTD TogNyoman TapayanaNoch keine Bewertungen
- Chapter 21 DigestionDokument96 SeitenChapter 21 DigestionJwnsbdhdNoch keine Bewertungen
- 2007 SaeDokument20 Seiten2007 Saelila1284Noch keine Bewertungen
- TRM05.03 Blunt Abdominal Trauma Guideline V2 - 08.17Dokument7 SeitenTRM05.03 Blunt Abdominal Trauma Guideline V2 - 08.17Erwin WibowoNoch keine Bewertungen
- Assignment Project ManagementDokument15 SeitenAssignment Project ManagementAhsanul Kabir SohanNoch keine Bewertungen
- BIRADS Poster 36x24in FDokument1 SeiteBIRADS Poster 36x24in FBk Del Riego100% (1)
- The Knight: Smoking and HealthDokument8 SeitenThe Knight: Smoking and Health健康生活園Healthy Life GardenNoch keine Bewertungen
- Dermatology Questions and Clinchers PDFDokument10 SeitenDermatology Questions and Clinchers PDFSahar nazNoch keine Bewertungen
- hnf41 Revised by Lau - To Be PrintDokument62 Seitenhnf41 Revised by Lau - To Be PrintJessa EsguerraNoch keine Bewertungen
- Sdo PM QF Sgod SHN 001 Students Health Card ElementaryDokument3 SeitenSdo PM QF Sgod SHN 001 Students Health Card ElementaryShiela E. EladNoch keine Bewertungen
- Pasteurelosis Neumónica (Mannheimiosis) BovinaDokument22 SeitenPasteurelosis Neumónica (Mannheimiosis) BovinaJesus Bustillo0% (1)
- 01 Serpentina Presentation PDFDokument27 Seiten01 Serpentina Presentation PDFabcNoch keine Bewertungen
- Differences Between Monozygotic and Dizygotic Twins: RD RDDokument11 SeitenDifferences Between Monozygotic and Dizygotic Twins: RD RDprism1702Noch keine Bewertungen
- SodaPDF-converted-lesson Plan of Cervical Cancer For ResearchDokument54 SeitenSodaPDF-converted-lesson Plan of Cervical Cancer For ResearchPatel KrimaNoch keine Bewertungen
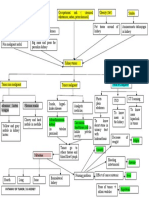
- Pathway Tumor GinjalDokument1 SeitePathway Tumor GinjalElizabeth VickiNoch keine Bewertungen
- Gastric Outlet ObstructionDokument35 SeitenGastric Outlet ObstructionsiddhantaNoch keine Bewertungen
- Phytochemistry, Antioxidant and Antibacterial Activities of Medicinal Plants - A Comparative StudyDokument12 SeitenPhytochemistry, Antioxidant and Antibacterial Activities of Medicinal Plants - A Comparative StudyRigotti BrNoch keine Bewertungen