Das könnte Ihnen auch gefallen
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (344)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (121)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (399)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (73)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- Comprehensive Soup ProjectDokument98 SeitenComprehensive Soup ProjectSachin Soni63% (8)
- A Project Report #1Dokument62 SeitenA Project Report #19415697349Noch keine Bewertungen
- Testing of Semifinished Products of Thermoplastics Bases - Indications Directive DVS 2201-1Dokument4 SeitenTesting of Semifinished Products of Thermoplastics Bases - Indications Directive DVS 2201-1OscarNoch keine Bewertungen
- Atomic Structure Worksheet: Name PeriodDokument4 SeitenAtomic Structure Worksheet: Name Periodapi-496534295100% (1)
- Riya Vishwakarma (2) 11Dokument92 SeitenRiya Vishwakarma (2) 119415697349Noch keine Bewertungen
- Jyoti Yadav 1474Dokument41 SeitenJyoti Yadav 14749415697349Noch keine Bewertungen
- Poonam Giri FINALDokument60 SeitenPoonam Giri FINAL9415697349Noch keine Bewertungen
- Jyoti Yadav Final 1Dokument76 SeitenJyoti Yadav Final 19415697349Noch keine Bewertungen
- Poonam Giri FINALDokument60 SeitenPoonam Giri FINAL9415697349Noch keine Bewertungen
- Jyoti Yadav Final 1Dokument76 SeitenJyoti Yadav Final 19415697349Noch keine Bewertungen
- Poonam Giri ChangeDokument81 SeitenPoonam Giri Change9415697349Noch keine Bewertungen
- Dr. Uday Khopkar: Consultant DermatopathologistDokument1 SeiteDr. Uday Khopkar: Consultant Dermatopathologist9415697349Noch keine Bewertungen
- D 17 14 Paper 3 III (Management) Inst Cbse Net Dec 2014Dokument32 SeitenD 17 14 Paper 3 III (Management) Inst Cbse Net Dec 2014DR.KUMAR PUNIT GOEL SIRNoch keine Bewertungen
- HmsDokument105 SeitenHms9415697349Noch keine Bewertungen
- PDF Mutual Funds Complete Project ReportDokument106 SeitenPDF Mutual Funds Complete Project Report9415697349Noch keine Bewertungen
- Ajay YadavDokument146 SeitenAjay Yadav9415697349Noch keine Bewertungen
- NTA UGC NET Management Paper 2 December 2013Dokument12 SeitenNTA UGC NET Management Paper 2 December 20139415697349Noch keine Bewertungen
- 15evidentary Value of ConfessionDokument23 Seiten15evidentary Value of ConfessionSomesh DixitNoch keine Bewertungen
- NTA UGC NET Management Paper 3 June 2014Dokument24 SeitenNTA UGC NET Management Paper 3 June 20149415697349Noch keine Bewertungen
- NTA UGC NET Management Paper 2 June 2014Dokument16 SeitenNTA UGC NET Management Paper 2 June 20149415697349Noch keine Bewertungen
- Banaras Hindu University: (Signature of The Research Scholar)Dokument2 SeitenBanaras Hindu University: (Signature of The Research Scholar)9415697349Noch keine Bewertungen
- The Living WorldDokument38 SeitenThe Living World9415697349Noch keine Bewertungen
- D 17 2netDokument24 SeitenD 17 2netNarendra JadhavNoch keine Bewertungen
- Banaras Hindu University: (Signature of The Research Scholar)Dokument2 SeitenBanaras Hindu University: (Signature of The Research Scholar)9415697349Noch keine Bewertungen
- 16 BibliographyDokument4 Seiten16 Bibliography9415697349Noch keine Bewertungen
- 14 Chapter 7Dokument32 Seiten14 Chapter 7ABHIJEETNoch keine Bewertungen
- Morphology of Flowering PlantsDokument62 SeitenMorphology of Flowering Plants9415697349Noch keine Bewertungen
- Animal Classification (Porifera-Echinodermata)Dokument164 SeitenAnimal Classification (Porifera-Echinodermata)9415697349Noch keine Bewertungen
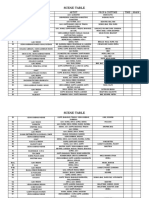
- Scene Table: Scene Location Artist Prop & Costume Time MarkDokument4 SeitenScene Table: Scene Location Artist Prop & Costume Time Mark9415697349Noch keine Bewertungen
- Dietary Intravention On Cardiac PatientsDokument45 SeitenDietary Intravention On Cardiac Patients9415697349Noch keine Bewertungen
- Dietary Intravention On Cardiac PatientsDokument45 SeitenDietary Intravention On Cardiac Patients9415697349Noch keine Bewertungen
- A Study On Ratio Analysis at HDFC BankDokument100 SeitenA Study On Ratio Analysis at HDFC Bank9415697349Noch keine Bewertungen
- Scene ChartDokument1 SeiteScene Chart9415697349Noch keine Bewertungen
- PS Ebook BagsPouches2 1116 HRDokument58 SeitenPS Ebook BagsPouches2 1116 HRGovindarajulu RNoch keine Bewertungen
- Tiling Checklist UpdatedDokument3 SeitenTiling Checklist UpdatedSayed Taimoor shahNoch keine Bewertungen
- Government of Canada Gouvernement Du CanadaDokument17 SeitenGovernment of Canada Gouvernement Du CanadaSaman BetkariNoch keine Bewertungen
- A Novel Procedure For Transient CFD Modeling of Basin Solar Stills, Coupling of Species and Energy EquationsDokument16 SeitenA Novel Procedure For Transient CFD Modeling of Basin Solar Stills, Coupling of Species and Energy EquationsAverroesNoch keine Bewertungen
- Cardiac AmyloidosisDokument3 SeitenCardiac AmyloidosisPrasad SrbNoch keine Bewertungen
- Profometer 5brochureDokument2 SeitenProfometer 5brochureLKBB Fakultas TeknikNoch keine Bewertungen
- NSF 型錄2Dokument2 SeitenNSF 型錄2Nermeen ElmelegaeNoch keine Bewertungen
- 1 PBDokument16 Seiten1 PBRaffi GigiNoch keine Bewertungen
- Colonel SandersDokument17 SeitenColonel SandersAmandaNoch keine Bewertungen
- Absenteeism in Public Sector: Presented byDokument25 SeitenAbsenteeism in Public Sector: Presented byPravin Rathod50% (2)
- The D - Block ElementsDokument30 SeitenThe D - Block ElementsNandya AristaNoch keine Bewertungen
- Patanjali CHP 1Dokument31 SeitenPatanjali CHP 1Prasad KadamNoch keine Bewertungen
- ErostorysDokument19 SeitenErostorysMayLiuNoch keine Bewertungen
- Ujian Diagnostik Ting 2 EnglishDokument9 SeitenUjian Diagnostik Ting 2 EnglishJ-Gie JaulahNoch keine Bewertungen
- Instructions For UseDokument14 SeitenInstructions For UseEddie UnivoNoch keine Bewertungen
- Steen Kamp 2021Dokument16 SeitenSteen Kamp 2021LARANSA SOLUNA GOGO SIMATUPANGNoch keine Bewertungen
- Radiation Hazards & Radiation ProtectionDokument62 SeitenRadiation Hazards & Radiation ProtectionGurupada JanaNoch keine Bewertungen
- TinyEYE Online Speech Therapy Media GuideDokument4 SeitenTinyEYE Online Speech Therapy Media GuideTinyEYE Therapy ServicesNoch keine Bewertungen
- 1stweek Intro Quanti Vs QualiDokument18 Seiten1stweek Intro Quanti Vs QualiHael LeighNoch keine Bewertungen
- Facebow Tech Spec Gen LRDokument1 SeiteFacebow Tech Spec Gen LRrojNoch keine Bewertungen
- MS Fresher HR DocumentDokument4 SeitenMS Fresher HR DocumentJahanvi KambojNoch keine Bewertungen
- Elephantgrass Bookchapter PDFDokument22 SeitenElephantgrass Bookchapter PDFMuhammad rifayNoch keine Bewertungen
- PAP and PAPE ReviewDokument9 SeitenPAP and PAPE ReviewYG1Noch keine Bewertungen
- Paracetamol DegradationDokument9 SeitenParacetamol DegradationTruyền Phạm MinhNoch keine Bewertungen
- PU-133AB - 規格GMXa spc 2022Dokument5 SeitenPU-133AB - 規格GMXa spc 2022Ý TrầnNoch keine Bewertungen
- Cell Organelles 2Dokument13 SeitenCell Organelles 2Sadeeq ur RahmanNoch keine Bewertungen
- Future Proofing Cities Toolkit by Craig Applegath 2012-03-01sm PDFDokument20 SeitenFuture Proofing Cities Toolkit by Craig Applegath 2012-03-01sm PDFJorge Fernández BaluarteNoch keine Bewertungen