Das könnte Ihnen auch gefallen
- 98ef337f-62a0-4dc9-9348-c8e8a2fdbf1cDokument41 Seiten98ef337f-62a0-4dc9-9348-c8e8a2fdbf1cThe SpiritNoch keine Bewertungen
- General English exam questionsDokument20 SeitenGeneral English exam questionsThe SpiritNoch keine Bewertungen
- Karnataka Drafts New Sports Policy to Promote Participation and ExcellenceDokument55 SeitenKarnataka Drafts New Sports Policy to Promote Participation and ExcellenceThe SpiritNoch keine Bewertungen
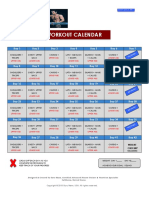
- 6week Shredded - Workout CalanderDokument1 Seite6week Shredded - Workout CalanderGopal KrishnaNoch keine Bewertungen
- Psi Civil KpscaaniDokument21 SeitenPsi Civil KpscaaniHruthik GowdaNoch keine Bewertungen
- PDFDokument850 SeitenPDFThe SpiritNoch keine Bewertungen
- BookletDokument12 SeitenBookletThe SpiritNoch keine Bewertungen
- Diet For Hostelier PDFDokument3 SeitenDiet For Hostelier PDFabhishek1709Noch keine Bewertungen
- Reference Document Athletics History at The OGDokument8 SeitenReference Document Athletics History at The OGThe SpiritNoch keine Bewertungen
- Paper-2 FPB 2018Dokument19 SeitenPaper-2 FPB 2018The SpiritNoch keine Bewertungen
- ManualtrDokument33 SeitenManualtrThe SpiritNoch keine Bewertungen
- Rules of Circle Style KabaddiDokument9 SeitenRules of Circle Style KabaddiMeiyappan MuniandyNoch keine Bewertungen
- Notification CISF Constable General Duty PostsDokument24 SeitenNotification CISF Constable General Duty PostsgopichandNoch keine Bewertungen
- 98ef337f-62a0-4dc9-9348-c8e8a2fdbf1cDokument41 Seiten98ef337f-62a0-4dc9-9348-c8e8a2fdbf1cThe SpiritNoch keine Bewertungen
- Facility Manual - IAAF Chapter 1&2Dokument140 SeitenFacility Manual - IAAF Chapter 1&2mericlon100% (8)
- Reference Document Athletics History at The OGDokument8 SeitenReference Document Athletics History at The OGThe SpiritNoch keine Bewertungen
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (399)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (73)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (344)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (120)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- 2006 Trauma Self-Assessment ExaminationDokument55 Seiten2006 Trauma Self-Assessment ExaminationHéctor Pando SánchezNoch keine Bewertungen
- Effect of Knee Position On Hip and Knee Torques During The Barbell SquatDokument5 SeitenEffect of Knee Position On Hip and Knee Torques During The Barbell SquatNicolás ManonniNoch keine Bewertungen
- Sae Technical Paper Series: Hector SerberDokument10 SeitenSae Technical Paper Series: Hector Serberashoksep11Noch keine Bewertungen
- Prosthetic Gait Analysis CICRDokument136 SeitenProsthetic Gait Analysis CICRyocondaariasNoch keine Bewertungen
- 647G556 All RU 03 2101w 4351042 enDokument32 Seiten647G556 All RU 03 2101w 4351042 enJuan CamiloNoch keine Bewertungen
- Tecnica de ThompsonDokument70 SeitenTecnica de Thompsonanibalpomi9351Noch keine Bewertungen
- Bjsports 2022 105495supp001Dokument17 SeitenBjsports 2022 105495supp001LUIS DAVID GARCIA BASTONoch keine Bewertungen
- Hamstring MuscleDokument8 SeitenHamstring MuscleMuhamad SdeqNoch keine Bewertungen
- Evaluationofthe Injuredrunner: Eric Magrum,, Robert P. WilderDokument15 SeitenEvaluationofthe Injuredrunner: Eric Magrum,, Robert P. WilderAndréia PicançoNoch keine Bewertungen
- Pathophysiology 7 EDITION: Concepts of Health and Disease: American Academy of Orthopedic Surgeons (Orthoinfo)Dokument2 SeitenPathophysiology 7 EDITION: Concepts of Health and Disease: American Academy of Orthopedic Surgeons (Orthoinfo)Justine Simeon lagunzadNoch keine Bewertungen
- Supp Hip OnlyDokument20 SeitenSupp Hip OnlyMark M. AlipioNoch keine Bewertungen
- Osteoarthritis: CausesDokument5 SeitenOsteoarthritis: CausesYahya i.nNoch keine Bewertungen
- Lower Extremity Anatomy ReviewDokument32 SeitenLower Extremity Anatomy Reviewkath-kath100% (1)
- Physical Education and Health 11Dokument50 SeitenPhysical Education and Health 11Janel Gel RamosNoch keine Bewertungen
- Skeletal Muscle PropertiesDokument7 SeitenSkeletal Muscle Propertiesrohitgaur210% (1)
- Kaltenbornmanualmobilizationsrs 150329041247 Conversion Gate01Dokument35 SeitenKaltenbornmanualmobilizationsrs 150329041247 Conversion Gate01Aaliyah ShaikhNoch keine Bewertungen
- Tibial Plateau Fracture Case ReportDokument6 SeitenTibial Plateau Fracture Case Reportapi-302580106Noch keine Bewertungen
- Genu RecurvatumDokument19 SeitenGenu Recurvatumapi-658182115Noch keine Bewertungen
- Triathlon Knee System: Surgical ProtocolDokument66 SeitenTriathlon Knee System: Surgical ProtocolJobin VargheseNoch keine Bewertungen
- ACL Reconstruction Rehab GuidelinesDokument4 SeitenACL Reconstruction Rehab GuidelinesIra AdventiaNoch keine Bewertungen
- 4 Year B.P.T. Subject: Physiotherapy in OrthopaedicsDokument36 Seiten4 Year B.P.T. Subject: Physiotherapy in OrthopaedicsNageswaraRoyal GovindugariNoch keine Bewertungen
- Stew Smith 6 Week Running PlanDokument15 SeitenStew Smith 6 Week Running PlanHenry GrimesNoch keine Bewertungen
- 11+ Running and Strength ExercisesDokument1 Seite11+ Running and Strength ExercisesArina MhtNoch keine Bewertungen
- Lecture 1-Introduction-Rationale For Corrective ExercisesDokument50 SeitenLecture 1-Introduction-Rationale For Corrective ExercisesGreg RoeNoch keine Bewertungen
- Williams Flexion Vs McKenzie Extension Exercises Low Back PainDokument3 SeitenWilliams Flexion Vs McKenzie Extension Exercises Low Back PainMasi KhanNoch keine Bewertungen
- Fibular Hemimelia FAQsDokument11 SeitenFibular Hemimelia FAQsLucila LugoNoch keine Bewertungen
- Sports Rehab: 5 Phases to Return Athletes to PlayDokument47 SeitenSports Rehab: 5 Phases to Return Athletes to PlayEira RajkumarNoch keine Bewertungen
- Injury Prevention 101 - 3 Ways To Prevent A Knee InjuryDokument8 SeitenInjury Prevention 101 - 3 Ways To Prevent A Knee InjuryAliNoch keine Bewertungen
- Handbook of Musculoskeletal Pain in The WorkplaceDokument511 SeitenHandbook of Musculoskeletal Pain in The WorkplaceJorge MartinsNoch keine Bewertungen
- Surface Anatomy of the Head, Neck, and ThoraxDokument57 SeitenSurface Anatomy of the Head, Neck, and ThoraxLavina SofiaNoch keine Bewertungen