Das könnte Ihnen auch gefallen
- CardiotocographyDokument51 SeitenCardiotocographyticticNoch keine Bewertungen
- NST CSTDokument9 SeitenNST CSTNadiya RashidNoch keine Bewertungen
- Role of Nurse MidwifeDokument31 SeitenRole of Nurse MidwiferekhamolNoch keine Bewertungen
- Welcome To The Morning SessionDokument20 SeitenWelcome To The Morning SessionGENERAL sharpNoch keine Bewertungen
- Abruption PacentaDokument6 SeitenAbruption PacentaKondapavuluru JyothiNoch keine Bewertungen
- Pain During PregnancyDokument32 SeitenPain During PregnancyDr. Jayesh PatidarNoch keine Bewertungen
- Jaundice in PregnancyDokument32 SeitenJaundice in PregnancyManoj Sankaranarayana100% (2)
- Metabolic Disorders in Pregnancy, Labour and Post PartumDokument45 SeitenMetabolic Disorders in Pregnancy, Labour and Post PartumNidhi SharmaNoch keine Bewertungen
- Effects of Maternal Drugs On The FetusDokument9 SeitenEffects of Maternal Drugs On The FetusJennifer DixonNoch keine Bewertungen
- Postpartum Hemorrhage (PPH) : Prakash Thakulla InternDokument38 SeitenPostpartum Hemorrhage (PPH) : Prakash Thakulla InternPrakash ThakullaNoch keine Bewertungen
- 27 Purpureal Venous Thrombosis and Pulmonary Embolism by Shambuling HebballiDokument14 Seiten27 Purpureal Venous Thrombosis and Pulmonary Embolism by Shambuling HebballiSamhitha Ayurvedic ChennaiNoch keine Bewertungen
- Cord Presentation and ProlapseDokument4 SeitenCord Presentation and ProlapseAnnapurna Dangeti100% (2)
- Partogram or PartographDokument5 SeitenPartogram or PartographCharo Flores100% (1)
- 26a. Post Partum HemorrhageDokument35 Seiten26a. Post Partum HemorrhageAubrey100% (1)
- Seminar On Complication of 3rd Stage PPHDokument13 SeitenSeminar On Complication of 3rd Stage PPHjuhi labana0% (1)
- 2nd Stage of LaborDokument79 Seiten2nd Stage of LaborJissa DaisonNoch keine Bewertungen
- Assessment of Fetal Well BeingDokument29 SeitenAssessment of Fetal Well Beingmalaika khanNoch keine Bewertungen
- Management of Cardiac Disease in PregnancyDokument7 SeitenManagement of Cardiac Disease in PregnancyMegavarnen Gobinathan100% (1)
- Physiological Changes During Second Stage of LabourDokument44 SeitenPhysiological Changes During Second Stage of LabourTami SelviNoch keine Bewertungen
- Physiology of 1st Stage of LaborDokument134 SeitenPhysiology of 1st Stage of LaborVijith.V.kumar50% (2)
- Nursing Education Format For Lesson Plan: Lourdes College of Nursing, Sidhi SadanDokument4 SeitenNursing Education Format For Lesson Plan: Lourdes College of Nursing, Sidhi SadanDelphy VargheseNoch keine Bewertungen
- Objectives of Aph:: To Define About APH. To List The Causes of APHDokument42 SeitenObjectives of Aph:: To Define About APH. To List The Causes of APHReena TyagiNoch keine Bewertungen
- PartographDokument33 SeitenPartographKathrynne Mendoza100% (1)
- Obg Res - PartographDokument20 SeitenObg Res - Partographmohapatra dev100% (1)
- Antenatal CareDokument50 SeitenAntenatal CareHari HardanaNoch keine Bewertungen
- High Risk Labour FinalDokument60 SeitenHigh Risk Labour FinalSusan HepziNoch keine Bewertungen
- Hormonal Cycle Lesson PlanDokument9 SeitenHormonal Cycle Lesson PlanGunaNoch keine Bewertungen
- 1 - Physiology of The Menstrual CycleDokument17 Seiten1 - Physiology of The Menstrual CycleMalak Ahmed 2295Noch keine Bewertungen
- Postnatal AssessmentDokument9 SeitenPostnatal Assessmentsaleha sultana100% (1)
- Exchange TransfusionDokument6 SeitenExchange TransfusionMonica SurduNoch keine Bewertungen
- Birth Injuries PDFDokument24 SeitenBirth Injuries PDFsaritha OrugantiNoch keine Bewertungen
- Asphyxia NeonatorumDokument34 SeitenAsphyxia NeonatorumListya Paramita100% (1)
- Amniotic Fluid EmbolismDokument19 SeitenAmniotic Fluid EmbolismSindhu JojoNoch keine Bewertungen
- CPDDokument9 SeitenCPDMeigy NitalessyNoch keine Bewertungen
- English Ii Assignment: Midwifery Management in Cephalopelvic DisproportionDokument14 SeitenEnglish Ii Assignment: Midwifery Management in Cephalopelvic DisproportionBintari Ancinonyx JubatusNoch keine Bewertungen
- Exchange Blood Transfusion 2Dokument15 SeitenExchange Blood Transfusion 2Sarah100% (1)
- Retained PlacentaDokument2 SeitenRetained PlacentaAmiraah MasriNoch keine Bewertungen
- Hypertensive Disorders in PregnancyDokument81 SeitenHypertensive Disorders in PregnancyarunshreerajendranNoch keine Bewertungen
- CervicitisDokument7 SeitenCervicitisElaisa Mae Delos SantosNoch keine Bewertungen
- Normal Labour: 4 Mbbs Class Esut College of Medicine 2013Dokument77 SeitenNormal Labour: 4 Mbbs Class Esut College of Medicine 2013nonny100% (1)
- Antenatal PreparationDokument26 SeitenAntenatal Preparationvaishali TMU studentNoch keine Bewertungen
- Genital Tract InjuriesDokument24 SeitenGenital Tract InjuriesManisha ThakurNoch keine Bewertungen
- Maternal, Morbidity, Mortality and Fertility RatesDokument18 SeitenMaternal, Morbidity, Mortality and Fertility Ratesmadhu.BNoch keine Bewertungen
- Heart Disease in Pregnancy: Mohana PreeshaDokument50 SeitenHeart Disease in Pregnancy: Mohana PreeshaChuks LeviNoch keine Bewertungen
- Management of PuerperiumDokument22 SeitenManagement of Puerperiumannu panchalNoch keine Bewertungen
- (11-13) Assess The Knowledge On Minor Ailments of Pregnancy-FormatDokument3 Seiten(11-13) Assess The Knowledge On Minor Ailments of Pregnancy-FormatMudasir Ahmad BhatNoch keine Bewertungen
- Assessment of The Fetal Well-BeingDokument85 SeitenAssessment of The Fetal Well-BeingAlphine DalgoNoch keine Bewertungen
- HysterectomyDokument2 SeitenHysterectomyJellou MacNoch keine Bewertungen
- Obstetric & Gynecology Nursing: Topic-Physiological Changes During LabourDokument54 SeitenObstetric & Gynecology Nursing: Topic-Physiological Changes During LabourBhumi ChouhanNoch keine Bewertungen
- Assessment of Intrauterine Fetal Well BeingDokument11 SeitenAssessment of Intrauterine Fetal Well Beingsagi mu100% (1)
- Obgyn Anemia in Pregnancy For UG ClassDokument35 SeitenObgyn Anemia in Pregnancy For UG ClassMunirathna ChandruNoch keine Bewertungen
- Revathi Papsmear ProcedureDokument50 SeitenRevathi Papsmear ProcedureRevathi DadamNoch keine Bewertungen
- Purperal InfectionsDokument69 SeitenPurperal InfectionsBeulah DasariNoch keine Bewertungen
- Labor and Birth Process 3 Stage & 4 Stage: RD THDokument23 SeitenLabor and Birth Process 3 Stage & 4 Stage: RD THبشائر حمادةNoch keine Bewertungen
- MINOR DISORDERS OF PREGNANCY FinalDokument6 SeitenMINOR DISORDERS OF PREGNANCY FinalChedupLepcha100% (7)
- Primary Uterine InertiaDokument4 SeitenPrimary Uterine InertiaTrisha Cayabyab100% (1)
- Pre & Post Operative Care of ChildrensDokument22 SeitenPre & Post Operative Care of Childrenscharan poonia100% (2)
- 3rd Stage of LabourDokument10 Seiten3rd Stage of LabourBhawna JoshiNoch keine Bewertungen
- CardiotocographyDokument46 SeitenCardiotocographyElisabeth F. OjhaNoch keine Bewertungen
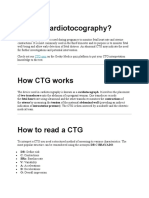
- What Is Cardiotocography?: Cardiotocography (CTG) Is Used During Pregnancy To Monitor Fetal Heart Rate and UterineDokument18 SeitenWhat Is Cardiotocography?: Cardiotocography (CTG) Is Used During Pregnancy To Monitor Fetal Heart Rate and Uterineمحمداحمد محمدنور ابايزيدNoch keine Bewertungen
- Vesicular MoleDokument27 SeitenVesicular MolePadmaNoch keine Bewertungen
- Hypoxic Ischemic EncephalopathyDokument10 SeitenHypoxic Ischemic EncephalopathyPadmaNoch keine Bewertungen
- Congenital Anomalies of GiDokument94 SeitenCongenital Anomalies of GiPadmaNoch keine Bewertungen
- Question BankDokument38 SeitenQuestion BankPadma100% (1)
- Abortion: DEFINITION-Abortion Is The Separation Partial orDokument77 SeitenAbortion: DEFINITION-Abortion Is The Separation Partial orPadmaNoch keine Bewertungen
- Non Stress TestDokument5 SeitenNon Stress TestPadma100% (1)
- Developing and Presenting A Research ProposalDokument17 SeitenDeveloping and Presenting A Research ProposalPadmaNoch keine Bewertungen
- Bonding NewDokument23 SeitenBonding NewPadmaNoch keine Bewertungen
- Semantic Diffrential Scale: IntroductionDokument7 SeitenSemantic Diffrential Scale: IntroductionPadmaNoch keine Bewertungen
- Semantic Diffrential Scale: IntroductionDokument4 SeitenSemantic Diffrential Scale: IntroductionPadmaNoch keine Bewertungen
- Postnatal ExcerciseDokument9 SeitenPostnatal ExcercisePadma75% (4)
- Multiple Pregnancy NOR Poster PDFDokument1 SeiteMultiple Pregnancy NOR Poster PDFbigbossNoch keine Bewertungen
- Introduction To Reproductive Health, Medical StudentsDokument25 SeitenIntroduction To Reproductive Health, Medical StudentsEli Zza KoiralaNoch keine Bewertungen
- Db05ec2db0dc5798725674a455fc (2) - 1Dokument2 SeitenDb05ec2db0dc5798725674a455fc (2) - 1Johnny PadernalNoch keine Bewertungen
- Sexual Life in Ancient Egypt IDokument2 SeitenSexual Life in Ancient Egypt INabil RoufailNoch keine Bewertungen
- All by Gyn Obst Depart PDFDokument27 SeitenAll by Gyn Obst Depart PDFRaouf Ra'fat Soliman100% (2)
- Chapter 07 Women Tell Their Personal StoriesDokument15 SeitenChapter 07 Women Tell Their Personal StoriessumomanusNoch keine Bewertungen
- Cover-Sblm Bab IDokument17 SeitenCover-Sblm Bab ISilmi RamdhaniatiNoch keine Bewertungen
- Research UkimDokument10 SeitenResearch UkimCyrus UrsuaNoch keine Bewertungen
- Fetal MonitoringDokument15 SeitenFetal MonitoringMelodia Turqueza GandezaNoch keine Bewertungen
- Philosophy of Sex Greta Christina ArticleDokument4 SeitenPhilosophy of Sex Greta Christina ArticleElenaNoch keine Bewertungen
- Lesson 2 Sexual SelfDokument7 SeitenLesson 2 Sexual SelfQueen MendozaNoch keine Bewertungen
- 2 Delivery Room Rotation 3Dokument74 Seiten2 Delivery Room Rotation 3Jianne CaloNoch keine Bewertungen
- Prenatal AssessmentDokument29 SeitenPrenatal AssessmentPaula Janine Barroga100% (1)
- 11 The Female Reproductive System Lec11 PDFDokument40 Seiten11 The Female Reproductive System Lec11 PDFTee bagNoch keine Bewertungen
- World Health Organization: Regional Office For The Western PacificDokument39 SeitenWorld Health Organization: Regional Office For The Western PacificlailyNoch keine Bewertungen
- 123456Dokument85 Seiten123456Mario ŠaravanjaNoch keine Bewertungen
- All Kinds of Sex ToysDokument4 SeitenAll Kinds of Sex ToyshousemouseNoch keine Bewertungen
- Works CitedDokument8 SeitenWorks Citedapi-313045940Noch keine Bewertungen
- AbortiondebateDokument4 SeitenAbortiondebateapi-354587776Noch keine Bewertungen
- MCN Finals NotesDokument287 SeitenMCN Finals NotesbabyboyNoch keine Bewertungen
- QnA - How Do Organisms ReproduceDokument5 SeitenQnA - How Do Organisms ReproduceArjan BhargavaNoch keine Bewertungen
- American Society For Reproductive MedicineDokument3 SeitenAmerican Society For Reproductive MedicineShanti Natalia NababanNoch keine Bewertungen
- The Morality of Abortion & RapeDokument20 SeitenThe Morality of Abortion & RapeDiane Sarino CabonceNoch keine Bewertungen
- OBSTETRICS - 1.05 Preconception and Prenatal Care (Dr. Famador) - 1Dokument7 SeitenOBSTETRICS - 1.05 Preconception and Prenatal Care (Dr. Famador) - 1Lchg KrvyNoch keine Bewertungen
- Clinical Focus CP 101Dokument3 SeitenClinical Focus CP 101Fely B. Balgoa100% (2)
- Obstetrics and GynecologyDokument36 SeitenObstetrics and GynecologyLeiNoch keine Bewertungen
- Manuskrip NewDokument4 SeitenManuskrip NewbaesootzuNoch keine Bewertungen
- Philosophy of SexualityDokument10 SeitenPhilosophy of SexualityJedda PunzalanNoch keine Bewertungen
- Kehamilan Dengan Hiv: Manggala Pasca WardhanaDokument38 SeitenKehamilan Dengan Hiv: Manggala Pasca WardhanaYudha SatriaNoch keine Bewertungen
- Cse CG Science Grades 3-10Dokument8 SeitenCse CG Science Grades 3-10Marlene Tagavilla-Felipe DiculenNoch keine Bewertungen