Das könnte Ihnen auch gefallen
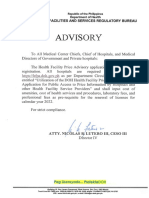
- dm2021 0261 Advisory On Provisional Primary Care CertificationDokument2 Seitendm2021 0261 Advisory On Provisional Primary Care CertificationJessa Mae75% (4)
- Change of PharmacistDokument1 SeiteChange of Pharmacistgrace taclobaoNoch keine Bewertungen
- Office of The SecretaryDokument11 SeitenOffice of The SecretaryAdrian Doctolero100% (5)
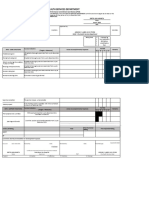
- Self-Assessment Form Official-ABTCDokument28 SeitenSelf-Assessment Form Official-ABTCJanice Villaroya Jarales-YusonNoch keine Bewertungen
- Rhu Citizen CharterDokument18 SeitenRhu Citizen CharteradrianNoch keine Bewertungen
- Presentation HEA OrientationDokument40 SeitenPresentation HEA OrientationEdrheyl Limbaga BiadnesNoch keine Bewertungen
- Form 5 - Rapid Health Assessment (MCI)Dokument1 SeiteForm 5 - Rapid Health Assessment (MCI)DELIVERY ROOMNoch keine Bewertungen
- Zero Reporting TemplateDokument1 SeiteZero Reporting Templatelance tabinas100% (2)
- Rabies Manual - MOP - 2019 Nov28 PDFDokument222 SeitenRabies Manual - MOP - 2019 Nov28 PDFSherylleen RodriguezNoch keine Bewertungen
- Doh Infection Prevention & Control Training Manual: Volume II For Health Facility AdministratorsDokument119 SeitenDoh Infection Prevention & Control Training Manual: Volume II For Health Facility AdministratorsAlex SanchezNoch keine Bewertungen
- Annual Operational Plan 2012 NarrativeDokument11 SeitenAnnual Operational Plan 2012 NarrativeArianne A ZamoraNoch keine Bewertungen
- QPMC Liph 2019Dokument69 SeitenQPMC Liph 2019JovelleAnneMondragonNoch keine Bewertungen
- Form 3-A - Rapid Health Assessment As of Jan 25 - 0Dokument3 SeitenForm 3-A - Rapid Health Assessment As of Jan 25 - 0Jessica Pineda- M ManalotoNoch keine Bewertungen
- Form 2a NTP Lab Request FormDokument2 SeitenForm 2a NTP Lab Request FormBe Nj100% (1)
- EO Epidemiology and SurveillanceDokument3 SeitenEO Epidemiology and SurveillanceJeffson100% (1)
- Tangalan Rural Health Unit Birthing Facility: Philippine Health Insurance CorporationDokument3 SeitenTangalan Rural Health Unit Birthing Facility: Philippine Health Insurance CorporationbenNoch keine Bewertungen
- AOP-2024-narrative FINALDokument66 SeitenAOP-2024-narrative FINALjasper manuelNoch keine Bewertungen
- Pidsr CifDokument17 SeitenPidsr CifAbraham Asto100% (4)
- Weekly Notifiable 2023Dokument1 SeiteWeekly Notifiable 2023johnmorts2014100% (1)
- Case Report Form For HFMDDokument2 SeitenCase Report Form For HFMDMendez RhuNoch keine Bewertungen
- Form 1 - HEARS Field Report As of Jan 25 - 0Dokument1 SeiteForm 1 - HEARS Field Report As of Jan 25 - 0Roanne Lagua100% (1)
- Policies and Procedure For Ensuring Quality of Sputum Microscopy ResultsDokument2 SeitenPolicies and Procedure For Ensuring Quality of Sputum Microscopy ResultsReinald Raven GuerreroNoch keine Bewertungen
- Birthing Facility IPCR RM Ver 1Dokument4 SeitenBirthing Facility IPCR RM Ver 1RvBombeta50% (2)
- All Case RateDokument91 SeitenAll Case RateTimothy Dycalle ManosNoch keine Bewertungen
- Annex B Konsulta ChecklistDokument8 SeitenAnnex B Konsulta ChecklistFret Ramirez Coronia RNNoch keine Bewertungen
- DOH Pregnancy Tracking FormDokument9 SeitenDOH Pregnancy Tracking FormEden VblagasyNoch keine Bewertungen
- AOP OPD Finalsituational and GAP AnalysisDokument2 SeitenAOP OPD Finalsituational and GAP AnalysisJennylyn GuadalupeNoch keine Bewertungen
- City Health Services Department: Individual Performance Commitment and Review (IPCR)Dokument8 SeitenCity Health Services Department: Individual Performance Commitment and Review (IPCR)Liecel Valdez100% (2)
- Case Investigation Forms - Pidsrmop3ed 1Dokument16 SeitenCase Investigation Forms - Pidsrmop3ed 1RHU Dupax del Sur100% (3)
- Aop 2022 New Form Blood ProgramDokument21 SeitenAop 2022 New Form Blood ProgramCHOLABORATORYNoch keine Bewertungen
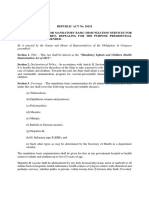
- R A 10152Dokument3 SeitenR A 10152Cesar Valera100% (4)
- Hfpa Advisory DCDokument5 SeitenHfpa Advisory DCldh pharmacyNoch keine Bewertungen
- Dianne A. Evangelista, M.D: Measuring and Learning Together Towards ResultsDokument59 SeitenDianne A. Evangelista, M.D: Measuring and Learning Together Towards ResultsKath DellosaNoch keine Bewertungen
- MedicalCertificate (Regular)Dokument1 SeiteMedicalCertificate (Regular)Gilbert Guzman TurarayNoch keine Bewertungen
- Bicol Regional HCPN Referral GuidelinesDokument56 SeitenBicol Regional HCPN Referral GuidelinesIT Department100% (4)
- Memorandum of Agreement PhilhealthDokument8 SeitenMemorandum of Agreement PhilhealthDeil L. NaveaNoch keine Bewertungen
- Central Visayas Health Referral System Clinical Referral FormDokument2 SeitenCentral Visayas Health Referral System Clinical Referral FormRjPinat0% (1)
- Loi MbfhiDokument11 SeitenLoi MbfhiAnsams Fats100% (2)
- Health Center IPCR RN Ver 1.1 (With Program Management)Dokument7 SeitenHealth Center IPCR RN Ver 1.1 (With Program Management)RvBombeta50% (2)
- Dog Bite Referral FormsDokument1 SeiteDog Bite Referral FormsConcepcion RHUNoch keine Bewertungen
- Prenatal Record FormDokument3 SeitenPrenatal Record FormIZABELLA BEATRICE ABANONoch keine Bewertungen
- Policies and Procedures in The Issuance of CertificatesDokument3 SeitenPolicies and Procedures in The Issuance of CertificatesREYNALDO DONIO100% (2)
- Form 6 - Rapid Health Assessment (Outbreak)Dokument1 SeiteForm 6 - Rapid Health Assessment (Outbreak)DELIVERY ROOMNoch keine Bewertungen
- ESR Verification FormDokument2 SeitenESR Verification Formlance tabinas83% (6)
- FAQs For Health FacilitiesDokument17 SeitenFAQs For Health FacilitiesPhilhealth ISDH SinaitNoch keine Bewertungen
- PIDSRDokument1 SeitePIDSRBilly Palma67% (6)
- PhilHealth Circular No. 0035, s.2013 Annex 2 List of Procedure Case RatesDokument98 SeitenPhilHealth Circular No. 0035, s.2013 Annex 2 List of Procedure Case RatesChrysanthus Herrera50% (2)
- Individual Performance Commitment Review (Ipcr) : Human Resources For Health Deployment Program (HRH-DP) 2018Dokument20 SeitenIndividual Performance Commitment Review (Ipcr) : Human Resources For Health Deployment Program (HRH-DP) 2018Bol McSafeNoch keine Bewertungen
- DOH Center For Health Development - I: Verification FormDokument2 SeitenDOH Center For Health Development - I: Verification FormGlessySeguillaBumanglag100% (4)
- DOH Memo No. 2019-0112 New and Renewal ApplicationDokument5 SeitenDOH Memo No. 2019-0112 New and Renewal ApplicationMenGuitar100% (3)
- DOH HFSRB QOP 01 Form1 3212019 postedDOH 1Dokument2 SeitenDOH HFSRB QOP 01 Form1 3212019 postedDOH 1Karina Santos89% (9)
- Form 2A. Laboratory Request and Result Form: To Be Filled Out by Health WorkerDokument1 SeiteForm 2A. Laboratory Request and Result Form: To Be Filled Out by Health WorkerJuvy Micutuan100% (2)
- Gene Xpert FormDokument1 SeiteGene Xpert FormAina HaravataNoch keine Bewertungen
- Gene Xpert FormDokument1 SeiteGene Xpert FormAina HaravataNoch keine Bewertungen
- Gene Xpert FormDokument1 SeiteGene Xpert FormAina HaravataNoch keine Bewertungen
- Form 4. TX Ipt Card v061416Dokument2 SeitenForm 4. TX Ipt Card v061416Emmanuel GorresNoch keine Bewertungen
- Lab LogDokument1 SeiteLab Logv2sc9kcsdgNoch keine Bewertungen
- 003 Pet-Ct Request Form Ikn - PDF - Google DriveDokument1 Seite003 Pet-Ct Request Form Ikn - PDF - Google DriveWapoyoii WapopocentauNoch keine Bewertungen
- TB DOTS Specimen - Releasing - FormDokument1 SeiteTB DOTS Specimen - Releasing - FormKim PeroNoch keine Bewertungen
- TB RequstDokument2 SeitenTB Requsttheviper12312Noch keine Bewertungen
- Introduction To Chemicals in MedicinesDokument5 SeitenIntroduction To Chemicals in MedicinesP balamoorthyNoch keine Bewertungen
- Novilyn C. Pataray BSN - Ii Pharyngitis: St. Paul College of Ilocos SurDokument1 SeiteNovilyn C. Pataray BSN - Ii Pharyngitis: St. Paul College of Ilocos SurCharina AubreyNoch keine Bewertungen
- NICE Guidelines 2009 - Borderline Personality Disorder Treatment and ManagementDokument41 SeitenNICE Guidelines 2009 - Borderline Personality Disorder Treatment and ManagementbechurinNoch keine Bewertungen
- PAMPHLETDokument2 SeitenPAMPHLETMarshin Thea CelociaNoch keine Bewertungen
- Leah Cronley ResumeDokument2 SeitenLeah Cronley Resumeapi-343462331Noch keine Bewertungen
- Cardiorenal Syndrome Referat Imam (BYS & EM)Dokument27 SeitenCardiorenal Syndrome Referat Imam (BYS & EM)Afrilia IntanNoch keine Bewertungen
- 2surgical Nursing-Chronic Illness and Older AdultsDokument6 Seiten2surgical Nursing-Chronic Illness and Older AdultsGedie RocamoraNoch keine Bewertungen
- Zoonotic Potentiality of Protozoa: Assignment Subject: ParasitologyDokument7 SeitenZoonotic Potentiality of Protozoa: Assignment Subject: ParasitologyArushi PatiyalNoch keine Bewertungen
- Concepts of DiseaseDokument55 SeitenConcepts of DiseaseKailash NagarNoch keine Bewertungen
- Anaemia in Dogs and Cats (Part 2) : Continuing EducationDokument6 SeitenAnaemia in Dogs and Cats (Part 2) : Continuing EducationAchmad NugrohoNoch keine Bewertungen
- Medication AdministrationDokument3 SeitenMedication AdministrationMonika SarmientoNoch keine Bewertungen
- Hypertensive Emergencies in The Emergency DepartmentDokument13 SeitenHypertensive Emergencies in The Emergency DepartmentLuis Lopez RevelesNoch keine Bewertungen
- PlagueDokument31 SeitenPlaguelulondon1Noch keine Bewertungen
- SIC (Carpio, Kurt Andrew)Dokument5 SeitenSIC (Carpio, Kurt Andrew)Kurt Andrew CarpioNoch keine Bewertungen
- Praposal DM-1Dokument117 SeitenPraposal DM-1sanjay sabdeNoch keine Bewertungen
- Understanding Psychopathology: The Study of Abnormal Psychology Is TheDokument34 SeitenUnderstanding Psychopathology: The Study of Abnormal Psychology Is TheJudyangaangan03Noch keine Bewertungen
- Patient Positioning (Sims, Orthopneic, Dorsal Recumbent) Guide (2020)Dokument28 SeitenPatient Positioning (Sims, Orthopneic, Dorsal Recumbent) Guide (2020)JOSHUA DICHOSO100% (1)
- Oxford Specialty Training Training in Obstetrics & GynaecologyDokument24 SeitenOxford Specialty Training Training in Obstetrics & GynaecologyPricope ElvisNoch keine Bewertungen
- Mental Health Case StudyDokument15 SeitenMental Health Case Studyapi-653708698Noch keine Bewertungen
- Medical AffixDokument6 SeitenMedical AffixOlib OlieNoch keine Bewertungen
- Nursing Care of The ElderlyDokument11 SeitenNursing Care of The ElderlySpislgal PhilipNoch keine Bewertungen
- Polymyalgia Rheumatic Symptoms Diagnosis and TreatmentDokument2 SeitenPolymyalgia Rheumatic Symptoms Diagnosis and TreatmentHas SimNoch keine Bewertungen
- 53 JMSCRDokument7 Seiten53 JMSCRAddinul FitryNoch keine Bewertungen
- Kansas College Immunization WaiverDokument1 SeiteKansas College Immunization WaiverDonnaNoch keine Bewertungen
- Vaccine Card - 20231120 - 175739 - 0000Dokument2 SeitenVaccine Card - 20231120 - 175739 - 0000MarilynNoch keine Bewertungen
- Name - IDDokument2 SeitenName - IDbasheNoch keine Bewertungen
- Uterine Prolapse in A Primigravid Woman JournalDokument13 SeitenUterine Prolapse in A Primigravid Woman JournalFadhlyanyNoch keine Bewertungen
- (Norma) Guia Fda CovidDokument14 Seiten(Norma) Guia Fda CovidJhovanaNoch keine Bewertungen
- AMA Retrospective AuditsDokument2 SeitenAMA Retrospective AuditsEma ForgacsNoch keine Bewertungen
- Advanced Practice Nursing Procedures 2º PDFDokument561 SeitenAdvanced Practice Nursing Procedures 2º PDFKey Guilbert100% (6)