Das könnte Ihnen auch gefallen
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (121)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (400)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2259)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (345)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (74)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- Signed Off - Personality Developent11 - q1 - m3 - Coping With Stress in Middle and Late Adolescence and The Powers of The Mind - v3 PDFDokument29 SeitenSigned Off - Personality Developent11 - q1 - m3 - Coping With Stress in Middle and Late Adolescence and The Powers of The Mind - v3 PDFRaniel John Avila Sampiano80% (5)
- Top 25 Test-Taking Tips, Suggestions & Strategies: WrongDokument5 SeitenTop 25 Test-Taking Tips, Suggestions & Strategies: WronglheanzNoch keine Bewertungen
- DLL Social ScienceDokument15 SeitenDLL Social ScienceMark Andris GempisawNoch keine Bewertungen
- AnswersDokument5 SeitenAnswersRyll Dela CruzNoch keine Bewertungen
- HYPOTHERMIADokument3 SeitenHYPOTHERMIARyll Dela CruzNoch keine Bewertungen
- Responsibility 1-Practices in Accordance With Legal Principles and The Code of Ethics in Making Personal and Professional JudgmentDokument13 SeitenResponsibility 1-Practices in Accordance With Legal Principles and The Code of Ethics in Making Personal and Professional JudgmentRyll Dela CruzNoch keine Bewertungen
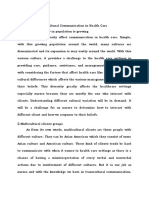
- B. Essay A. Explain The Transcultural Communication in Health CareDokument2 SeitenB. Essay A. Explain The Transcultural Communication in Health CareRyll Dela CruzNoch keine Bewertungen
- Disaster Post ImpactDokument51 SeitenDisaster Post ImpactRyll Dela CruzNoch keine Bewertungen
- Chapter 5Dokument16 SeitenChapter 5Ryll Dela CruzNoch keine Bewertungen
- Attachment 0Dokument23 SeitenAttachment 0Ryll Dela CruzNoch keine Bewertungen
- Pregnancy: The Three Steps of Pregnancy 1. Ovulation: The Ovary Releases A Mature EggDokument3 SeitenPregnancy: The Three Steps of Pregnancy 1. Ovulation: The Ovary Releases A Mature EggRyll Dela CruzNoch keine Bewertungen
- Getting Out of Your Comfort ZoneDokument14 SeitenGetting Out of Your Comfort ZoneRyll Dela CruzNoch keine Bewertungen
- Chapter 4Dokument35 SeitenChapter 4Ryll Dela CruzNoch keine Bewertungen
- Vii. Drug Study: Generic Name Indication Action Adverse Reaction Contraidication Patient EducationDokument3 SeitenVii. Drug Study: Generic Name Indication Action Adverse Reaction Contraidication Patient EducationRyll Dela CruzNoch keine Bewertungen
- Performing IV CannulationDokument1 SeitePerforming IV CannulationRyll Dela CruzNoch keine Bewertungen
- Arcanobacterium Haemolyticum, Chlamydia Pneumoniae, Mycoplasma PneumoniaeDokument21 SeitenArcanobacterium Haemolyticum, Chlamydia Pneumoniae, Mycoplasma PneumoniaeRyll Dela CruzNoch keine Bewertungen
- Planning: Presentation by Obiora AngelaDokument7 SeitenPlanning: Presentation by Obiora AngelaRyll Dela CruzNoch keine Bewertungen
- The Health Care Provider Has Ordered A Magnetic Resonance Imaging (MRI) Study To BeDokument1 SeiteThe Health Care Provider Has Ordered A Magnetic Resonance Imaging (MRI) Study To BeRyll Dela CruzNoch keine Bewertungen
- A Case Study On Pleural Effusion: University of Luzon College of Nursing Dagupan, PangasinanDokument13 SeitenA Case Study On Pleural Effusion: University of Luzon College of Nursing Dagupan, PangasinanRyll Dela CruzNoch keine Bewertungen
- Bone CancerDokument26 SeitenBone CancerRyll Dela CruzNoch keine Bewertungen
- Summary Product Charecteristics: Rabies Vaccine For Human Use, (Vero-Cell) Freeze-Dried (Speeda Vaccine)Dokument4 SeitenSummary Product Charecteristics: Rabies Vaccine For Human Use, (Vero-Cell) Freeze-Dried (Speeda Vaccine)Ryll Dela CruzNoch keine Bewertungen
- 82 83 1 PB 1Dokument5 Seiten82 83 1 PB 1Ryll Dela CruzNoch keine Bewertungen
- How To Motivate Students in Learning English As A Second LanguageDokument2 SeitenHow To Motivate Students in Learning English As A Second LanguagebulliinaNoch keine Bewertungen
- (Or How Blah-Blah-Blah Has Gradually Taken Over Our Lives) Dan RoamDokument18 Seiten(Or How Blah-Blah-Blah Has Gradually Taken Over Our Lives) Dan RoamVictoria AdhityaNoch keine Bewertungen
- Linking Extracurricular Programming To Academic Achievement: Wiio Benefits and Why?Dokument28 SeitenLinking Extracurricular Programming To Academic Achievement: Wiio Benefits and Why?Laeeq ZafarNoch keine Bewertungen
- Four Mystery DramasDokument370 SeitenFour Mystery Dramastberni92Noch keine Bewertungen
- B1 Writing Intermediate 1Dokument2 SeitenB1 Writing Intermediate 1Mohamed NasirNoch keine Bewertungen
- Lesson Plan For Math 1Dokument6 SeitenLesson Plan For Math 1Mary ChemlyNoch keine Bewertungen
- According To MaslowDokument4 SeitenAccording To Maslowfaithparagoso9Noch keine Bewertungen
- 070 - Searching For Effective Neural Network Architectures For Heart Murmur Detection From PhonocardiogramDokument4 Seiten070 - Searching For Effective Neural Network Architectures For Heart Murmur Detection From PhonocardiogramDalana PasinduNoch keine Bewertungen
- Bartle Elements of Integration and Lebesgue MeasureDokument20 SeitenBartle Elements of Integration and Lebesgue MeasureAlejandro FandiñoNoch keine Bewertungen
- Drohvalenko - Ea - 2021 - First Finding of Triploid in Mozh RiverDokument7 SeitenDrohvalenko - Ea - 2021 - First Finding of Triploid in Mozh RiverErlkonigNoch keine Bewertungen
- Unit Vi Natural Language ProcessingDokument2 SeitenUnit Vi Natural Language ProcessingNikita AgrawalNoch keine Bewertungen
- Landon AlexanderDokument6 SeitenLandon Alexanderapi-455881201Noch keine Bewertungen
- Features of 21st Century HRD and Training ProgramsDokument9 SeitenFeatures of 21st Century HRD and Training Programstvglacaba1213100% (1)
- CST 47 TeacherDokument56 SeitenCST 47 TeacherElena DavalosNoch keine Bewertungen
- Arjun Emf CVDokument2 SeitenArjun Emf CVArjun PrasadNoch keine Bewertungen
- Comparing Numbers (2021 - 06 - 19 01 - 35 - 12 UTC) (2021 - 08 - 06 04 - 51 - 25 UTC)Dokument3 SeitenComparing Numbers (2021 - 06 - 19 01 - 35 - 12 UTC) (2021 - 08 - 06 04 - 51 - 25 UTC)ALLinOne BlogNoch keine Bewertungen
- TheraDokument4 SeitenTheramaircusNoch keine Bewertungen
- Karakter Anak Usia Dini Yang Tinggal Di Daerah Pesisir PantaiDokument12 SeitenKarakter Anak Usia Dini Yang Tinggal Di Daerah Pesisir PantaiMoh. Ibnu UbaidillahNoch keine Bewertungen
- Module 2 AssignmentDokument15 SeitenModule 2 AssignmentFatima Usman100% (3)
- Kalvi Tholaikatchi New TimetableDokument2 SeitenKalvi Tholaikatchi New TimetableTamilaruviNoch keine Bewertungen
- Should Students Consider Taking A Gap Year Before Starting UniversityDokument20 SeitenShould Students Consider Taking A Gap Year Before Starting Universityzahra321Noch keine Bewertungen
- Seva Bharathi Kishori Vikas - EnglishDokument15 SeitenSeva Bharathi Kishori Vikas - EnglishSevaBharathiTelanganaNoch keine Bewertungen
- SN Key Result Area Key Task Performance Standards 1 Teaching and LearningDokument2 SeitenSN Key Result Area Key Task Performance Standards 1 Teaching and LearningrajksdNoch keine Bewertungen
- Regular Schedule For Senior HighDokument4 SeitenRegular Schedule For Senior HighCecille IdjaoNoch keine Bewertungen
- Edited - Reagan Horn - Ap Research Inquiry Proposal FormDokument2 SeitenEdited - Reagan Horn - Ap Research Inquiry Proposal Formapi-645342010Noch keine Bewertungen
- FE Final ExamDokument2 SeitenFE Final Examabraham kassahunNoch keine Bewertungen
- Sisyphus - Journal of Education - Vol 5, Issue 1Dokument121 SeitenSisyphus - Journal of Education - Vol 5, Issue 1Instituto de Educação da Universidade de LisboaNoch keine Bewertungen