Das könnte Ihnen auch gefallen
- TB Update 2016Dokument67 SeitenTB Update 2016Nila hermawatiNoch keine Bewertungen
- Bell KJ Thesis 2 PDFDokument84 SeitenBell KJ Thesis 2 PDFlifeinhimNoch keine Bewertungen
- Kindergarten Physical Education LessonDokument7 SeitenKindergarten Physical Education Lessonapi-185987237Noch keine Bewertungen
- Presentasi TBDokument18 SeitenPresentasi TBAristoteles MillerNoch keine Bewertungen
- TB Usia Sekolah & RemajaDokument80 SeitenTB Usia Sekolah & RemajaDinaNoch keine Bewertungen
- Pengenalan TB, Diagnosis, Dan Pengobatannya FKM 2019Dokument47 SeitenPengenalan TB, Diagnosis, Dan Pengobatannya FKM 2019yuly rahmawatiNoch keine Bewertungen
- Acierto, Dyvi Karen T. Catanyag, Hussein E. Ignacio, Karen G. Palanca, AriesDokument32 SeitenAcierto, Dyvi Karen T. Catanyag, Hussein E. Ignacio, Karen G. Palanca, AriesBea MagnoNoch keine Bewertungen
- Journal ReviewDokument16 SeitenJournal Reviewnur ulfahNoch keine Bewertungen
- 07-08 Fmui Student DotsDokument59 Seiten07-08 Fmui Student Dotsdiklat pkckramatjatiNoch keine Bewertungen
- 12.uji Tuberkulin Dan Pencegahan TB Pada AnakDokument29 Seiten12.uji Tuberkulin Dan Pencegahan TB Pada AnakAndriano Arie WibowoNoch keine Bewertungen
- Uji Tuberkulin Dan Pencegahan TB Pada Anak: Ketikan Kuliah DR - Finny Fitry Yani, Sp.ADokument29 SeitenUji Tuberkulin Dan Pencegahan TB Pada Anak: Ketikan Kuliah DR - Finny Fitry Yani, Sp.AAndriano Arie WibowoNoch keine Bewertungen
- M1. B3. U3. Communicable Diseases - 2Dokument91 SeitenM1. B3. U3. Communicable Diseases - 2prashantNoch keine Bewertungen
- Tuberkulosis Pada Anak: Dr. Afdal, Spa. M.BiomedDokument48 SeitenTuberkulosis Pada Anak: Dr. Afdal, Spa. M.BiomedKekenYenniNoch keine Bewertungen
- IDS - Tuberculosis (Dr. Sy)Dokument5 SeitenIDS - Tuberculosis (Dr. Sy)Renrenz PayumoNoch keine Bewertungen
- Pediatric Tuberculosis: Specimen Collection For Analysis Sputum Specimens - Used in OlderDokument3 SeitenPediatric Tuberculosis: Specimen Collection For Analysis Sputum Specimens - Used in OldernadiahNoch keine Bewertungen
- 6 COMMUNICABLE DISEASES Nies PDokument14 Seiten6 COMMUNICABLE DISEASES Nies PMontero, Ma. Cecilia - BSN 3-BNoch keine Bewertungen
- Pathology of TuberculosisDokument51 SeitenPathology of TuberculosisChristopher YoungNoch keine Bewertungen
- B5M2 - Respiratory System (Case 5)Dokument4 SeitenB5M2 - Respiratory System (Case 5)JNoch keine Bewertungen
- TB PedDokument34 SeitenTB PedSebastián NovoaNoch keine Bewertungen
- Host Defenses Part 1 - Cellular & TB - 250Dokument5 SeitenHost Defenses Part 1 - Cellular & TB - 250Matt CloudNoch keine Bewertungen
- 1 s2.0 S1198743X1461822X MainDokument5 Seiten1 s2.0 S1198743X1461822X MainPUPUT PUJIANTINoch keine Bewertungen
- Tuberculosis: Clinical PharmacyDokument20 SeitenTuberculosis: Clinical PharmacyEllen Shayne Pajigal FloridaNoch keine Bewertungen
- Cong InfDokument72 SeitenCong InffarazNoch keine Bewertungen
- Pediatric Drug Sensitive TBDokument69 SeitenPediatric Drug Sensitive TBEnita ChaniagoNoch keine Bewertungen
- Li Ulin LBM 1 IPEDokument16 SeitenLi Ulin LBM 1 IPEUlin NuhaNoch keine Bewertungen
- Paradigma Pemeriksaan TBDokument40 SeitenParadigma Pemeriksaan TBTengku AdriansyahNoch keine Bewertungen
- Tuberculosis or TBDokument8 SeitenTuberculosis or TBJ Russel DichosoNoch keine Bewertungen
- TuberculosisDokument2 SeitenTuberculosisamr amerNoch keine Bewertungen
- Congenital Tuberculosis A Review ArticleDokument5 SeitenCongenital Tuberculosis A Review ArticleMasita RochsalehaNoch keine Bewertungen
- Laboratory Diagnosis of Mycobacterium Tuberculosis Infection and Disease in ChildrenDokument8 SeitenLaboratory Diagnosis of Mycobacterium Tuberculosis Infection and Disease in ChildrenFaradilla FirdausaNoch keine Bewertungen
- Congenital Tuberculosis Presenting As Sepsis SyndromeDokument5 SeitenCongenital Tuberculosis Presenting As Sepsis SyndromeTwhieNoch keine Bewertungen
- TB Paru FK UncenDokument66 SeitenTB Paru FK UncenAndira Trianingrum TukanNoch keine Bewertungen
- Bagian Kesehatan Anak: Mycobacterium Tuberculosis. PenyakitDokument2 SeitenBagian Kesehatan Anak: Mycobacterium Tuberculosis. PenyakitAlverina Ode NifakiNoch keine Bewertungen
- TB Ped 2019Dokument14 SeitenTB Ped 2019Edgar ronán Cabrera moralesNoch keine Bewertungen
- Pediatric TB UpdateDokument55 SeitenPediatric TB UpdateDenaya Tika ReskiaNoch keine Bewertungen
- Tuberkulosis: Febtarini. R, Dr. SP - PK Ikt-Fkuwks Senin, 22-Oktober-2018Dokument20 SeitenTuberkulosis: Febtarini. R, Dr. SP - PK Ikt-Fkuwks Senin, 22-Oktober-2018bayu kuberaNoch keine Bewertungen
- 10 Communicable Disease Control Program IDokument9 Seiten10 Communicable Disease Control Program IJennica JaoNoch keine Bewertungen
- Journal Homepage: - : IntroductionDokument5 SeitenJournal Homepage: - : IntroductionIJAR JOURNALNoch keine Bewertungen
- Paediatric Tuberculosis: Best PracticeDokument7 SeitenPaediatric Tuberculosis: Best PracticeIndah IndrianiNoch keine Bewertungen
- The Correlation of Foxp3 - Gene and Regulator - 2020 - Journal of Clinical TuberDokument7 SeitenThe Correlation of Foxp3 - Gene and Regulator - 2020 - Journal of Clinical TuberKarina ChristantoNoch keine Bewertungen
- I-SPOT - TB Presentation - enDokument23 SeitenI-SPOT - TB Presentation - endanang setiawanNoch keine Bewertungen
- TuberculosisDokument53 SeitenTuberculosisDaniel JaymeNoch keine Bewertungen
- TuberculosisDokument35 SeitenTuberculosisAmr KhayyalNoch keine Bewertungen
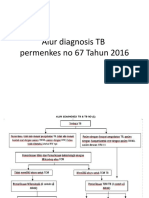
- Alur Diagnosis TB Permenkes No 67 Tahun 2016Dokument7 SeitenAlur Diagnosis TB Permenkes No 67 Tahun 2016nunuksumiartiNoch keine Bewertungen
- RNTCPDokument46 SeitenRNTCPdarshitkotadiya2553Noch keine Bewertungen
- Cabalgada World TB Day Health Education PlanDokument7 SeitenCabalgada World TB Day Health Education PlanHaroldJohnCabalgadaNoch keine Bewertungen
- Tuberculous Meningitis: Basal Cistern Enhancement Pattern On CT ImagingDokument9 SeitenTuberculous Meningitis: Basal Cistern Enhancement Pattern On CT ImagingDeei RizalNoch keine Bewertungen
- Nastiti N. Rahajoe: Department of Child Health Medical School University of Indonesia JakartaDokument40 SeitenNastiti N. Rahajoe: Department of Child Health Medical School University of Indonesia JakartaSaniaty TuankottaNoch keine Bewertungen
- Teaching Plan For TBDokument5 SeitenTeaching Plan For TBakritiNoch keine Bewertungen
- Contact Investigation and IPT - WS PRA KONIKA 2017Dokument27 SeitenContact Investigation and IPT - WS PRA KONIKA 2017Rifny Hanifah SyawalNoch keine Bewertungen
- NTB ppt-1Dokument76 SeitenNTB ppt-1yazgariNoch keine Bewertungen
- Pedia Pulmo 3Dokument48 SeitenPedia Pulmo 3Sven OrdanzaNoch keine Bewertungen
- Clinical Microbiology (24 - 11 - 21)Dokument19 SeitenClinical Microbiology (24 - 11 - 21)Arthur YanezNoch keine Bewertungen
- Early Human Development: Elizabeth Whittaker, Beate KampmannDokument5 SeitenEarly Human Development: Elizabeth Whittaker, Beate KampmannTwhieNoch keine Bewertungen
- Tuberculosis Latente NEJMDokument10 SeitenTuberculosis Latente NEJMBiblioteca Médica CDS -HGZcMF-1Noch keine Bewertungen
- Msir Jawaid Mmedical: MicrobiologyDokument28 SeitenMsir Jawaid Mmedical: Microbiologykashif89Noch keine Bewertungen
- The 7 Immunizable Diseases AreDokument6 SeitenThe 7 Immunizable Diseases AreGladie Ann Dela RosaNoch keine Bewertungen
- Pulmonary TuberculosisDokument68 SeitenPulmonary TuberculosisNur Arthirah Raden67% (3)
- M2 AP 1 Pag26-28Dokument4 SeitenM2 AP 1 Pag26-28ANGEL LUGO TRAMPENoch keine Bewertungen
- 930954246tb ClassificationDokument1 Seite930954246tb ClassificationJeane Irish EgotNoch keine Bewertungen
- Hepatitis B Virus and Liver DiseaseVon EverandHepatitis B Virus and Liver DiseaseJia-Horng KaoNoch keine Bewertungen
- Acute Flaccid Paralysis: Case Investigation FormDokument2 SeitenAcute Flaccid Paralysis: Case Investigation FormPaul Angelo E. Caliva0% (1)
- Disorders of Blood Pressure Regulation - 10Dokument31 SeitenDisorders of Blood Pressure Regulation - 10Cres Padua QuinzonNoch keine Bewertungen
- Acute Gastroenteritis REPORTDokument11 SeitenAcute Gastroenteritis REPORTMelai Barneso Leal100% (1)
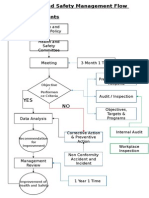
- Health and Safety FlowDokument6 SeitenHealth and Safety Flowzaki0304Noch keine Bewertungen
- Ventilation Health Guide COVID 19Dokument25 SeitenVentilation Health Guide COVID 19Carlos Valle TurciosNoch keine Bewertungen
- Epidemiology Principles - Slide 1Dokument8 SeitenEpidemiology Principles - Slide 1Tamia WilliamsNoch keine Bewertungen
- NBHS 1104 Topic 2Dokument18 SeitenNBHS 1104 Topic 2hema angleNoch keine Bewertungen
- Online Class During PandemicDokument6 SeitenOnline Class During PandemicShariz DinoyoNoch keine Bewertungen
- An Analysis On The Level of Satisfaction Brought by The School CanteenDokument81 SeitenAn Analysis On The Level of Satisfaction Brought by The School Canteenkyla manapat100% (5)
- R08 HE3C32 TIE PLN HS 0004 Emergency Response PlanDokument27 SeitenR08 HE3C32 TIE PLN HS 0004 Emergency Response PlanHafiz ZameerNoch keine Bewertungen
- Metastase Bone DiseaseDokument20 SeitenMetastase Bone DiseasedrkurniatiNoch keine Bewertungen
- Preparation For Child BirthDokument41 SeitenPreparation For Child BirthAngelica ErguizaNoch keine Bewertungen
- The Occupational Brain A Theory of Human NatureDokument6 SeitenThe Occupational Brain A Theory of Human NatureJoaquin OlivaresNoch keine Bewertungen
- The Geisha Secret Ancient Dating Rituals Proven To Win A Modern Mans Heart Hanako Z LibraryDokument165 SeitenThe Geisha Secret Ancient Dating Rituals Proven To Win A Modern Mans Heart Hanako Z LibraryMarius CristianNoch keine Bewertungen
- How To Read A CTG: What Is Cardiotocography?Dokument11 SeitenHow To Read A CTG: What Is Cardiotocography?Rinothja RajaratnamNoch keine Bewertungen
- Revision Sistematica Preparacion A La Practica Dental 2018Dokument9 SeitenRevision Sistematica Preparacion A La Practica Dental 2018Chris MartinNoch keine Bewertungen
- Gubra DIO Mouse Data FlyerDokument2 SeitenGubra DIO Mouse Data FlyerGabrielaMirelaAlexeNoch keine Bewertungen
- 2012 Costs Fact Sheet Version Alzheimers AssociationDokument2 Seiten2012 Costs Fact Sheet Version Alzheimers AssociationynottripNoch keine Bewertungen
- Vaccination Lesson PlanDokument2 SeitenVaccination Lesson Planapi-517831630Noch keine Bewertungen
- How To Get Rid of Panic Attacks Without MedicationDokument20 SeitenHow To Get Rid of Panic Attacks Without MedicationmidnightgrNoch keine Bewertungen
- Metatarsalgia Rehabilitation ExercisesDokument2 SeitenMetatarsalgia Rehabilitation ExercisesnatsNoch keine Bewertungen
- Drug Study OxytocinDokument3 SeitenDrug Study OxytocinSheena Marie M. TarleNoch keine Bewertungen
- NCM 104 10 Herbal MedicinesDokument4 SeitenNCM 104 10 Herbal MedicinesElleNoch keine Bewertungen
- IvabradineDokument30 SeitenIvabradinepashaNoch keine Bewertungen
- Vacuum Extraction Is An Artificial LaborDokument6 SeitenVacuum Extraction Is An Artificial LaborYuriko_L7Noch keine Bewertungen
- OHS-PR-09-03-F02 RISK ASSESSMENT For INSTALLATION OF WALL MOUNTED JIB CRANEDokument21 SeitenOHS-PR-09-03-F02 RISK ASSESSMENT For INSTALLATION OF WALL MOUNTED JIB CRANEmohammed tofiqNoch keine Bewertungen
- Trauma-Informed Care For Behavioral Health Service ProvidersDokument159 SeitenTrauma-Informed Care For Behavioral Health Service ProvidersAlguémNoch keine Bewertungen
- Jesse Smith Letter of ReccDokument1 SeiteJesse Smith Letter of Reccapi-510425013Noch keine Bewertungen