Das könnte Ihnen auch gefallen
- Herbal MedicineDokument5 SeitenHerbal MedicineYessaminNoch keine Bewertungen
- Healthcare: Analysis of Anxiety Levels of Nursing Students Because of E-Learning During The COVID-19 PandemicDokument11 SeitenHealthcare: Analysis of Anxiety Levels of Nursing Students Because of E-Learning During The COVID-19 PandemicYessaminNoch keine Bewertungen
- Jonald Cortez Mandap: Address: 811 Purok 4 Cansinala, Apalit, Pampanga Contact Number: 09756008984Dokument1 SeiteJonald Cortez Mandap: Address: 811 Purok 4 Cansinala, Apalit, Pampanga Contact Number: 09756008984YessaminNoch keine Bewertungen
- Male and FemaleDokument1 SeiteMale and FemaleYessaminNoch keine Bewertungen
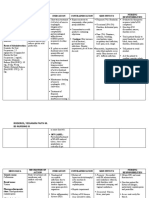
- NCP (Pre-Operative) : Assessment Nursing Diagnosis Planning Nursing Intervention Rationale Evaluation Subjective CuesDokument2 SeitenNCP (Pre-Operative) : Assessment Nursing Diagnosis Planning Nursing Intervention Rationale Evaluation Subjective CuesYessamin100% (1)
- Ian Carlo C. Mandap Grade 7-St. LukeDokument1 SeiteIan Carlo C. Mandap Grade 7-St. LukeYessaminNoch keine Bewertungen
- GadDokument1 SeiteGadYessaminNoch keine Bewertungen
- Drug Study (Covid Case)Dokument5 SeitenDrug Study (Covid Case)YessaminNoch keine Bewertungen
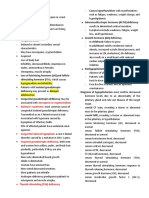
- Micropenis or Cryptorchidism Kallman's Syndrome:: Thyroid-Stimulating (TSH) DeficiencyDokument4 SeitenMicropenis or Cryptorchidism Kallman's Syndrome:: Thyroid-Stimulating (TSH) DeficiencyYessamin Paith RoderosNoch keine Bewertungen
- Group 2 QuizDokument1 SeiteGroup 2 QuizYessaminNoch keine Bewertungen
- Overview of The CaseDokument3 SeitenOverview of The CaseYessaminNoch keine Bewertungen
- A Case ofDokument55 SeitenA Case ofYessaminNoch keine Bewertungen
- Medical Surgical NursingDokument1 SeiteMedical Surgical NursingYessaminNoch keine Bewertungen
- HERNIORRHAPYDokument2 SeitenHERNIORRHAPYYessaminNoch keine Bewertungen
- Data Gathering ProceduresDokument2 SeitenData Gathering ProceduresYessaminNoch keine Bewertungen
- Fluid Volume Overload ScriptDokument3 SeitenFluid Volume Overload ScriptYessaminNoch keine Bewertungen
- Gi NCP ScriptDokument1 SeiteGi NCP ScriptYessaminNoch keine Bewertungen
- Complete Blood CountDokument5 SeitenComplete Blood CountYessaminNoch keine Bewertungen
- DISCUSSIO1Dokument2 SeitenDISCUSSIO1YessaminNoch keine Bewertungen
- DiscussionDokument2 SeitenDiscussionYessaminNoch keine Bewertungen
- Risk For Infection Related To Failure To Avoid Pathogen Secondary To Exposure To COVID-19Dokument2 SeitenRisk For Infection Related To Failure To Avoid Pathogen Secondary To Exposure To COVID-19Yessamin Paith Roderos100% (1)
- Metric System EquivalentsDokument2 SeitenMetric System EquivalentsYessaminNoch keine Bewertungen
- College of Nursing: City of Malolos, BulacanDokument255 SeitenCollege of Nursing: City of Malolos, BulacanYessamin Paith RoderosNoch keine Bewertungen
- Endoscopic Procedure (Nursing Responsibilities)Dokument4 SeitenEndoscopic Procedure (Nursing Responsibilities)YessaminNoch keine Bewertungen
- DisDokument2 SeitenDisYessaminNoch keine Bewertungen
- Subjective Cues: Independent: On The: "Nahihirapa N Ako Huminga" AsDokument5 SeitenSubjective Cues: Independent: On The: "Nahihirapa N Ako Huminga" AsYessaminNoch keine Bewertungen
- Subjective Cues: Independent: On The: "Nahihirapa N Ako Huminga" AsDokument5 SeitenSubjective Cues: Independent: On The: "Nahihirapa N Ako Huminga" AsYessaminNoch keine Bewertungen
- Vital Signs Checklist 1Dokument4 SeitenVital Signs Checklist 1YessaminNoch keine Bewertungen
- 2 Ethical IssuesDokument86 Seiten2 Ethical IssuesYessaminNoch keine Bewertungen
- MJDT Scholars FormDokument1 SeiteMJDT Scholars FormYessaminNoch keine Bewertungen
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (344)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (399)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (73)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2259)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (120)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- Manajemen Nyeri Dengan DexketoprofenDokument27 SeitenManajemen Nyeri Dengan Dexketoprofenmaya santiNoch keine Bewertungen
- Body Mri Protocols: Abdomen PelvisDokument35 SeitenBody Mri Protocols: Abdomen PelvisManuCastroNoch keine Bewertungen
- Complications of Injectable Fillers, Part 2: Vascular ComplicationsDokument17 SeitenComplications of Injectable Fillers, Part 2: Vascular ComplicationsIsabel JiménezNoch keine Bewertungen
- Severity of Acute Stress Symptoms Child Age 11 To 17Dokument3 SeitenSeverity of Acute Stress Symptoms Child Age 11 To 17brown_chocolate87643Noch keine Bewertungen
- NycoCard Brochure 01Dokument2 SeitenNycoCard Brochure 01TimNoch keine Bewertungen
- International Olympic Committee (IOC) Consensus Statement On Relative Energy de Ficiency in Sport (RED-S) : 2018 UpdateDokument16 SeitenInternational Olympic Committee (IOC) Consensus Statement On Relative Energy de Ficiency in Sport (RED-S) : 2018 UpdateNicol TrujilloNoch keine Bewertungen
- Disinfection & Sterilization 2Dokument49 SeitenDisinfection & Sterilization 2YasminNoch keine Bewertungen
- Kode Pintar Icd 10Dokument48 SeitenKode Pintar Icd 10Glory Stephanie Tesalonika Supit100% (2)
- Ngo Module 1aDokument7 SeitenNgo Module 1aAmiel simon NgoNoch keine Bewertungen
- Sost - Funda - Medication AdministrationDokument8 SeitenSost - Funda - Medication AdministrationKYLE SABAYNoch keine Bewertungen
- LTM SenseDokument6 SeitenLTM SenseNabilla MerdikaNoch keine Bewertungen
- Anatomy Review: Blood Vessel Structure & Function: Page 1. Introduction Page 2. GoalsDokument6 SeitenAnatomy Review: Blood Vessel Structure & Function: Page 1. Introduction Page 2. GoalsUta Provinsiana SukmaraNoch keine Bewertungen
- CBCT - Cone Beam Computed TomographyDokument11 SeitenCBCT - Cone Beam Computed TomographyandreemNoch keine Bewertungen
- The Effects of Estrogens and ProgesteroneDokument7 SeitenThe Effects of Estrogens and ProgesteroneTinke WinkeNoch keine Bewertungen
- Textbook of Clinical NeurologyDokument374 SeitenTextbook of Clinical Neurologykanuparthyj100% (9)
- Antibiotik Dan Antiseptik Saluran KemihDokument14 SeitenAntibiotik Dan Antiseptik Saluran KemihPuterinugraha Wanca ApatyaNoch keine Bewertungen
- Acute Flaccid ParalysisDokument4 SeitenAcute Flaccid ParalysisZharah RuzNoch keine Bewertungen
- ANATOM 128 Brochure-ReDokument8 SeitenANATOM 128 Brochure-ReAli MirzaNoch keine Bewertungen
- Malandain Leo Pharmacotherapy of Sexual AddictionDokument8 SeitenMalandain Leo Pharmacotherapy of Sexual AddictionSergio De PanfilisNoch keine Bewertungen
- EMERGING DEASESE CDC - Pdf-Version PDFDokument156 SeitenEMERGING DEASESE CDC - Pdf-Version PDFanyNoch keine Bewertungen
- So BulananDokument89 SeitenSo BulananHeru Tri WibowoNoch keine Bewertungen
- Ocular Drug Delivery: Dr. Herman J. WoerdenbagDokument32 SeitenOcular Drug Delivery: Dr. Herman J. Woerdenbagitung23Noch keine Bewertungen
- Introduction To The Three-Dimensional Scoliosis Treatment According To SchrothDokument6 SeitenIntroduction To The Three-Dimensional Scoliosis Treatment According To SchrothIvens NakagawaNoch keine Bewertungen
- Rule 15Dokument2 SeitenRule 15begenyolNoch keine Bewertungen
- Pub Personality TypeDokument16 SeitenPub Personality TypeYessika Adelwin NataliaNoch keine Bewertungen
- Nauclea Latifolia: A Medicinal, Economic and Pharmacological ReviewDokument19 SeitenNauclea Latifolia: A Medicinal, Economic and Pharmacological ReviewMichael Kwesi BaahNoch keine Bewertungen
- Article With BhajanDokument4 SeitenArticle With BhajanBibek SutradharNoch keine Bewertungen
- BVGH Global Health Primer 10dec07Dokument72 SeitenBVGH Global Health Primer 10dec07hst939Noch keine Bewertungen
- Ic PDFDokument409 SeitenIc PDFandreeamandoiuNoch keine Bewertungen
- FLCCC Alliance I RECOVER Management Protocol For Long Haul COVID 19 SyndromeDokument3 SeitenFLCCC Alliance I RECOVER Management Protocol For Long Haul COVID 19 SyndromeAizaz ul HaqNoch keine Bewertungen