Das könnte Ihnen auch gefallen
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (894)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (587)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (344)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (119)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (399)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2219)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (265)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (73)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- AgraLi The Low Chloride Liquid Fertilizer For Sensitive Crops enDokument2 SeitenAgraLi The Low Chloride Liquid Fertilizer For Sensitive Crops enASHNoch keine Bewertungen
- Lester Desjarlais Inquest Parts I and IIDokument108 SeitenLester Desjarlais Inquest Parts I and IIJames Turner100% (1)
- DWG TrueView DWG Convert Conversion ReportDokument1 SeiteDWG TrueView DWG Convert Conversion ReportCosmin CinciNoch keine Bewertungen
- Multiple Trip Permit Conditions: To Transport Large And/or Heavy ArticlesDokument2 SeitenMultiple Trip Permit Conditions: To Transport Large And/or Heavy ArticlesJulian TremontNoch keine Bewertungen
- Material SpecificationDokument2 SeitenMaterial SpecificationJulian TremontNoch keine Bewertungen
- Material SpecificationDokument2 SeitenMaterial SpecificationJulian TremontNoch keine Bewertungen
- General Notes: Ma Ma MoDokument2 SeitenGeneral Notes: Ma Ma MoJulian TremontNoch keine Bewertungen
- MV 2195Dokument2 SeitenMV 2195Julian TremontNoch keine Bewertungen
- Single Trip Application: No YesDokument1 SeiteSingle Trip Application: No YesJulian TremontNoch keine Bewertungen
- Single Trip Permit General Conditions: To Transport Mobile Homes And/or Modular Building SectionsDokument2 SeitenSingle Trip Permit General Conditions: To Transport Mobile Homes And/or Modular Building SectionsJulian TremontNoch keine Bewertungen
- Raw Forest and Agricultural Products Weight Limitations ChartDokument2 SeitenRaw Forest and Agricultural Products Weight Limitations ChartJulian TremontNoch keine Bewertungen
- Motorcycle School BondDokument1 SeiteMotorcycle School BondJulian TremontNoch keine Bewertungen
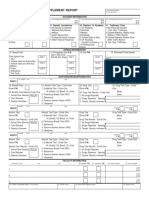
- Motor Vehicle Fatal Supplement Report: Unit 1Dokument2 SeitenMotor Vehicle Fatal Supplement Report: Unit 1Julian TremontNoch keine Bewertungen
- EeeeeDokument2 SeitenEeeeeJulian TremontNoch keine Bewertungen
- Motor Vehicle Salvage Dealer or Recycler Two Year License ApplicationDokument2 SeitenMotor Vehicle Salvage Dealer or Recycler Two Year License ApplicationJulian TremontNoch keine Bewertungen
- Single Trip Permit Application: Section A - Customer Please Print Clearly or TypeDokument1 SeiteSingle Trip Permit Application: Section A - Customer Please Print Clearly or TypeJulian TremontNoch keine Bewertungen
- Responsibility Agreement: Distribution: White - Agency Pink - Person Taking CustodyDokument1 SeiteResponsibility Agreement: Distribution: White - Agency Pink - Person Taking CustodyJulian TremontNoch keine Bewertungen
- Oversize/Overweight Single Trip Permit InformationDokument1 SeiteOversize/Overweight Single Trip Permit InformationJulian TremontNoch keine Bewertungen
- MV 2195Dokument2 SeitenMV 2195Julian TremontNoch keine Bewertungen
- dt1037 PDFDokument1 Seitedt1037 PDFJulian TremontNoch keine Bewertungen
- MV 2489Dokument1 SeiteMV 2489Julian TremontNoch keine Bewertungen
- PSWebinar 032014Dokument39 SeitenPSWebinar 032014Julian TremontNoch keine Bewertungen
- Wisconsin DOT Driver School BondDokument1 SeiteWisconsin DOT Driver School BondJulian TremontNoch keine Bewertungen
- MV 2085Dokument1 SeiteMV 2085Julian TremontNoch keine Bewertungen
- Design of Gantry ShedsDokument4 SeitenDesign of Gantry ShedsJulian TremontNoch keine Bewertungen
- Certificate Templates For Word2Dokument1 SeiteCertificate Templates For Word2Julian TremontNoch keine Bewertungen
- Certificate Templates For Word4Dokument1 SeiteCertificate Templates For Word4Julian TremontNoch keine Bewertungen
- Tri P10Dokument10 SeitenTri P10Dvd Davide La CruzNoch keine Bewertungen
- Tax Calculation 2010Dokument9 SeitenTax Calculation 2010Julian TremontNoch keine Bewertungen
- PumpDokument4 SeitenPumpJulian TremontNoch keine Bewertungen
- Diseño Electrico - I.E.N° 11134 OkDokument52 SeitenDiseño Electrico - I.E.N° 11134 OkJulian TremontNoch keine Bewertungen
- Incident Reports 2017-2019Dokument8 SeitenIncident Reports 2017-2019Buddzilla FranciscoNoch keine Bewertungen
- Sampling Methods GuideDokument35 SeitenSampling Methods GuideKim RamosNoch keine Bewertungen
- 11 Foods That Lower Cholesterol: Foods That Make Up A Low Cholesterol Diet Can Help Reduce High LevelsDokument3 Seiten11 Foods That Lower Cholesterol: Foods That Make Up A Low Cholesterol Diet Can Help Reduce High Levelsaj dancel marcosNoch keine Bewertungen
- Stress Amongst Healthcare Professionals and Migrant Workers During Covid-19 PandemicDokument6 SeitenStress Amongst Healthcare Professionals and Migrant Workers During Covid-19 PandemicIJAR JOURNALNoch keine Bewertungen
- Class 7 PolityDokument10 SeitenClass 7 PolityNakka nikithaNoch keine Bewertungen
- Care Plan SummaryDokument5 SeitenCare Plan Summaryapi-541785084Noch keine Bewertungen
- Fluid Management in The Critically Ill: Jean-Louis VincentDokument6 SeitenFluid Management in The Critically Ill: Jean-Louis VincentFlorentina NadisaNoch keine Bewertungen
- STP 1560-2013Dokument346 SeitenSTP 1560-2013HieuHTNoch keine Bewertungen
- Bmjopen 2017 016402Dokument6 SeitenBmjopen 2017 016402Ćatke TkećaNoch keine Bewertungen
- Anthrax (Woolsesters Disease, Malignant Edema) What Is Anthrax?Dokument3 SeitenAnthrax (Woolsesters Disease, Malignant Edema) What Is Anthrax?rvanguardiaNoch keine Bewertungen
- Remote Working A Dream Job British English Advanced c1 c2 GroupDokument5 SeitenRemote Working A Dream Job British English Advanced c1 c2 GroupNick ManishevNoch keine Bewertungen
- Voyeuristic Disorder SymptomsDokument7 SeitenVoyeuristic Disorder SymptomsgoyaNoch keine Bewertungen
- Full Plate Diet BookDokument164 SeitenFull Plate Diet BookScarlettNyx100% (4)
- 67166-Apvma Veterinary Medicines Technical Report TemplateDokument42 Seiten67166-Apvma Veterinary Medicines Technical Report Templateali aimanNoch keine Bewertungen
- ASP ProductsDokument33 SeitenASP ProductsSerghei Barba100% (1)
- Undulating Periodization For BodybuildingDokument24 SeitenUndulating Periodization For BodybuildingPete Puza89% (9)
- Liquefied Gas Tanker Familiarisation Course: Operational & Support LevelDokument60 SeitenLiquefied Gas Tanker Familiarisation Course: Operational & Support LevelAlpha OmegaNoch keine Bewertungen
- Rabia PDFDokument22 SeitenRabia PDFLadybirdNoch keine Bewertungen
- Boy Scouts Lipa City Investiture CampDokument1 SeiteBoy Scouts Lipa City Investiture CampAndro Brendo VillapandoNoch keine Bewertungen
- Respiration 3... Pulmonary Function TestsDokument26 SeitenRespiration 3... Pulmonary Function Testsapi-19641337Noch keine Bewertungen
- Complete VaccinationDokument2 SeitenComplete VaccinationNgoo NwosuNoch keine Bewertungen
- 2012 Bringing Our Dying HomeDokument68 Seiten2012 Bringing Our Dying HomeendofliferesearchNoch keine Bewertungen
- Informed Consent and Release, Waiver, and Quitclaim: Know All Men by These PresentsDokument2 SeitenInformed Consent and Release, Waiver, and Quitclaim: Know All Men by These PresentsRobee Camille Desabelle-SumatraNoch keine Bewertungen
- Bio-Oil® Product ManualDokument60 SeitenBio-Oil® Product ManualguitarristaclasicosdnNoch keine Bewertungen
- Questionnaire/interview Guide Experiences of Checkpoint Volunteers During The Covid-19 PandemicDokument16 SeitenQuestionnaire/interview Guide Experiences of Checkpoint Volunteers During The Covid-19 PandemicKrisna Criselda SimbreNoch keine Bewertungen
- Cardiovascular NotesDokument18 SeitenCardiovascular NotesCathy SantosNoch keine Bewertungen