Das könnte Ihnen auch gefallen
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- Innovations in Land AdministrationDokument66 SeitenInnovations in Land AdministrationSanjawe KbNoch keine Bewertungen
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- Functions of Commercial Banks: Primary and Secondary FunctionsDokument3 SeitenFunctions of Commercial Banks: Primary and Secondary FunctionsPavan Kumar SuralaNoch keine Bewertungen
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
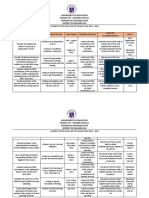
- Action Plan Lis 2021-2022Dokument3 SeitenAction Plan Lis 2021-2022Vervie BingalogNoch keine Bewertungen
- Hayashi Q Econometica 82Dokument16 SeitenHayashi Q Econometica 82Franco VenesiaNoch keine Bewertungen
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (400)
- ACIS - Auditing Computer Information SystemDokument10 SeitenACIS - Auditing Computer Information SystemErwin Labayog MedinaNoch keine Bewertungen
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
- Pneumatic Fly Ash Conveying0 PDFDokument1 SeitePneumatic Fly Ash Conveying0 PDFnjc6151Noch keine Bewertungen
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- Building and Other Construction Workers Act 1996Dokument151 SeitenBuilding and Other Construction Workers Act 1996Rajesh KodavatiNoch keine Bewertungen
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- Efs151 Parts ManualDokument78 SeitenEfs151 Parts ManualRafael VanegasNoch keine Bewertungen
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
- Separation PayDokument3 SeitenSeparation PayMalen Roque Saludes100% (1)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- Historical Development of AccountingDokument25 SeitenHistorical Development of AccountingstrifehartNoch keine Bewertungen
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- Cabling and Connection System PDFDokument16 SeitenCabling and Connection System PDFLyndryl ProvidoNoch keine Bewertungen
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- Algorithmique Et Programmation en C: Cours Avec 200 Exercices CorrigésDokument298 SeitenAlgorithmique Et Programmation en C: Cours Avec 200 Exercices CorrigésSerges KeouNoch keine Bewertungen
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- Methodical Pointing For Work of Students On Practical EmploymentDokument32 SeitenMethodical Pointing For Work of Students On Practical EmploymentVidhu YadavNoch keine Bewertungen
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (74)
- Forecasting of Nonlinear Time Series Using Artificial Neural NetworkDokument9 SeitenForecasting of Nonlinear Time Series Using Artificial Neural NetworkranaNoch keine Bewertungen
- Walmart, Amazon, EbayDokument2 SeitenWalmart, Amazon, EbayRELAKU GMAILNoch keine Bewertungen
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- 4109 CPC For ExamDokument380 Seiten4109 CPC For ExamMMM-2012Noch keine Bewertungen
- 18 - PPAG-100-HD-C-001 - s018 (VBA03C013) - 0 PDFDokument1 Seite18 - PPAG-100-HD-C-001 - s018 (VBA03C013) - 0 PDFSantiago GarciaNoch keine Bewertungen
- 90FF1DC58987 PDFDokument9 Seiten90FF1DC58987 PDFfanta tasfayeNoch keine Bewertungen
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (345)
- QUIZ Group 1 Answer KeyDokument3 SeitenQUIZ Group 1 Answer KeyJames MercadoNoch keine Bewertungen
- The Art of Blues SolosDokument51 SeitenThe Art of Blues SolosEnrique Maldonado100% (8)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2259)
- Amerisolar AS 7M144 HC Module Specification - CompressedDokument2 SeitenAmerisolar AS 7M144 HC Module Specification - CompressedMarcus AlbaniNoch keine Bewertungen
- Bajaj Allianz InsuranceDokument93 SeitenBajaj Allianz InsuranceswatiNoch keine Bewertungen
- ATPDraw 5 User Manual UpdatesDokument51 SeitenATPDraw 5 User Manual UpdatesdoniluzNoch keine Bewertungen
- Are Groups and Teams The Same Thing? An Evaluation From The Point of Organizational PerformanceDokument6 SeitenAre Groups and Teams The Same Thing? An Evaluation From The Point of Organizational PerformanceNely Noer SofwatiNoch keine Bewertungen
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- Danby Dac5088m User ManualDokument12 SeitenDanby Dac5088m User ManualElla MariaNoch keine Bewertungen
- Datasheet Qsfp28 PAMDokument43 SeitenDatasheet Qsfp28 PAMJonny TNoch keine Bewertungen
- A. The Machine's Final Recorded Value Was P1,558,000Dokument7 SeitenA. The Machine's Final Recorded Value Was P1,558,000Tawan VihokratanaNoch keine Bewertungen
- CodebreakerDokument3 SeitenCodebreakerwarrenNoch keine Bewertungen
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (121)
- 2021S-EPM 1163 - Day-11-Unit-8 ProcMgmt-AODADokument13 Seiten2021S-EPM 1163 - Day-11-Unit-8 ProcMgmt-AODAehsan ershadNoch keine Bewertungen
- FIRE FIGHTING ROBOT (Mini Project)Dokument21 SeitenFIRE FIGHTING ROBOT (Mini Project)Hisham Kunjumuhammed100% (2)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)