Das könnte Ihnen auch gefallen
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- Facial Nerve Preservation During Giant Mandibular Tumor SurgeryDokument3 SeitenFacial Nerve Preservation During Giant Mandibular Tumor SurgeryRuc NguyenNoch keine Bewertungen
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (399)
- Facial Nerve Danger ZonesDokument4 SeitenFacial Nerve Danger ZonesRuc NguyenNoch keine Bewertungen
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- Hohman 2013Dokument6 SeitenHohman 2013AditiNoch keine Bewertungen
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (894)
- Anatomical Considerations To Prevent Facial Nerve InjuryDokument10 SeitenAnatomical Considerations To Prevent Facial Nerve InjuryRuc NguyenNoch keine Bewertungen
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- Facial Nerve Injury and Repair A Practical Review For Cutaneous SurgeryDokument18 SeitenFacial Nerve Injury and Repair A Practical Review For Cutaneous SurgeryRuc NguyenNoch keine Bewertungen
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- A Combined ALT Flap, ALT Flap, and Vascularized Lliac Bone Graft For A Full Thickness Defect of The Mental RegionDokument6 SeitenA Combined ALT Flap, ALT Flap, and Vascularized Lliac Bone Graft For A Full Thickness Defect of The Mental RegionRuc NguyenNoch keine Bewertungen
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- Anatomic Variations of The Marginal Mandibular NerveDokument4 SeitenAnatomic Variations of The Marginal Mandibular NerveRuc NguyenNoch keine Bewertungen
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- A Follow - Up Study On Functional and Aesthetic Recipient and Donor Site OutcomeDokument10 SeitenA Follow - Up Study On Functional and Aesthetic Recipient and Donor Site OutcomeRuc NguyenNoch keine Bewertungen
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (587)
- Single Stage Soft Tissue and Extensor Tendon Reconstruction of UpperDokument4 SeitenSingle Stage Soft Tissue and Extensor Tendon Reconstruction of UpperRuc NguyenNoch keine Bewertungen
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (265)
- Further Experience With Adipofascial ALT ApDokument6 SeitenFurther Experience With Adipofascial ALT ApRuc NguyenNoch keine Bewertungen
- Skillet Good & GreasyDokument1 SeiteSkillet Good & Greasyilya neviditsinNoch keine Bewertungen
- 220200320sathiya PrakashDokument95 Seiten220200320sathiya Prakashpriya selvaraj100% (1)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- Intrinsic and Extrinsic Hand MusclesDokument2 SeitenIntrinsic and Extrinsic Hand MusclesSerge KhelemskyNoch keine Bewertungen
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (73)
- Anatomy of Upper LimbDokument112 SeitenAnatomy of Upper LimbUzma KhanNoch keine Bewertungen
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (344)
- Paper 8Dokument40 SeitenPaper 8Francisco Javier Luza Ramos100% (1)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- Shoulder ConditionsDokument8 SeitenShoulder ConditionsCarlos GonzalesNoch keine Bewertungen
- Therapeutic Exercise Movement AssignmentDokument4 SeitenTherapeutic Exercise Movement Assignmentapi-272092949Noch keine Bewertungen
- Physical Examination of The Shoulder FinalDokument28 SeitenPhysical Examination of The Shoulder FinalAndinNoch keine Bewertungen
- Anatomy Concept Book AtfDokument246 SeitenAnatomy Concept Book AtfRishi ShekharNoch keine Bewertungen
- Anatomy Review of Extreme TiesDokument65 SeitenAnatomy Review of Extreme Tiesskihard0404749Noch keine Bewertungen
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- Anatomi Regio Antebrachii Et Manus (Lo 1)Dokument24 SeitenAnatomi Regio Antebrachii Et Manus (Lo 1)Warni PutriNoch keine Bewertungen
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2219)
- Kin 4KK3 - L8 Shoulder FoundationsDokument6 SeitenKin 4KK3 - L8 Shoulder FoundationsYurNoch keine Bewertungen
- (Ebook - Martial Arts) Kung Fu MovementsDokument17 Seiten(Ebook - Martial Arts) Kung Fu Movementsrq100% (1)
- Miyamoto 2010 JBJS Current Concepts Review Distal-Biceps-Tendon-Injuries PDFDokument12 SeitenMiyamoto 2010 JBJS Current Concepts Review Distal-Biceps-Tendon-Injuries PDFKuozram No MasNoch keine Bewertungen
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- Netter Atlas UL ChartsDokument4 SeitenNetter Atlas UL ChartsJUSASB100% (1)
- Swimming AnatomyDokument21 SeitenSwimming AnatomyArwin Aguirre MirandaNoch keine Bewertungen
- Palmar SpaceDokument22 SeitenPalmar Spaceamobiabdulmuiz08Noch keine Bewertungen
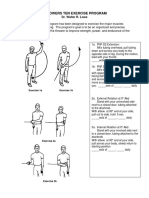
- LP 1throwers - Ten - Exercises - 2010 PDFDokument5 SeitenLP 1throwers - Ten - Exercises - 2010 PDFClaudiaNoch keine Bewertungen
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (119)
- Kinesiology Elbow Joint PDFDokument8 SeitenKinesiology Elbow Joint PDFRozyNoch keine Bewertungen
- Snorlax Template PDFDokument1 SeiteSnorlax Template PDFshaira alliah de castroNoch keine Bewertungen
- Tension Band Wiring For Avulsion Fracture of Olecranon in A Dog PDFDokument2 SeitenTension Band Wiring For Avulsion Fracture of Olecranon in A Dog PDFvetarifNoch keine Bewertungen
- Terrible Triad - ElbowDokument96 SeitenTerrible Triad - ElbowWasim R. IssaNoch keine Bewertungen
- Antagonistic PairsDokument1 SeiteAntagonistic PairsKasam ANoch keine Bewertungen
- A Radiologist's Guide To: Wrist AlignmentDokument35 SeitenA Radiologist's Guide To: Wrist Alignmentsisiramohan100% (1)
- Preventing shoulder injuries in overhead athletesDokument9 SeitenPreventing shoulder injuries in overhead athletesLeonardiniNoch keine Bewertungen
- 2008-Distal Radius Morphometry in The Malaysian PopulationDokument4 Seiten2008-Distal Radius Morphometry in The Malaysian PopulationPongnarin JiamwatthanachaiNoch keine Bewertungen
- Examination of The Joints and ExtremitiesDokument66 SeitenExamination of The Joints and Extremitiesapi-25914483Noch keine Bewertungen
- Audley v. Walsh - Sponge Ball Manipulation (1947)Dokument16 SeitenAudley v. Walsh - Sponge Ball Manipulation (1947)EugeneBurger100% (5)
- Intro To Ortho Anatomy PDFDokument55 SeitenIntro To Ortho Anatomy PDFlanghalilafaNoch keine Bewertungen
- De Quervain's Tenosynovitis (Guide To The Diagnosis of Work-Related Musculoskeletal Disorders, 2) (PDFDrive)Dokument39 SeitenDe Quervain's Tenosynovitis (Guide To The Diagnosis of Work-Related Musculoskeletal Disorders, 2) (PDFDrive)audiNoch keine Bewertungen
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)