Das könnte Ihnen auch gefallen
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
- Educaation For Gerontic NursingDokument1 SeiteEducaation For Gerontic NursingTiara KusumaNoch keine Bewertungen
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- Geriatrics, Gerontology, GeronticDokument5 SeitenGeriatrics, Gerontology, GeronticTsaabitah AnwarNoch keine Bewertungen
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- Disturbed Sleep PatternDokument4 SeitenDisturbed Sleep PatternTsaabitah AnwarNoch keine Bewertungen
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- Nursing Care Plan For Patient With Excessive FluidDokument11 SeitenNursing Care Plan For Patient With Excessive FluidTsaabitah AnwarNoch keine Bewertungen
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
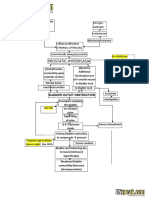
- Benign Prostatic Hyperplasia BPH Pathophysiology Schematic Diagram PDFDokument2 SeitenBenign Prostatic Hyperplasia BPH Pathophysiology Schematic Diagram PDFgailNoch keine Bewertungen
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (399)
- Science 2ND Grading Human Reproductive SystemDokument5 SeitenScience 2ND Grading Human Reproductive SystemYouls TorNoch keine Bewertungen
- MennaDokument7 SeitenMennaDr. Mohammad JamaliNoch keine Bewertungen
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (73)
- Checklist (PapSmear)Dokument5 SeitenChecklist (PapSmear)Sinung BawonoNoch keine Bewertungen
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- Basic Clinical Laboratory Techniques 6Th Edition Estridge Solutions Manual Full Chapter PDFDokument60 SeitenBasic Clinical Laboratory Techniques 6Th Edition Estridge Solutions Manual Full Chapter PDFflorenceronaldoxo0100% (11)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
- Urinary Tract InfectionDokument3 SeitenUrinary Tract InfectionHo Yong WaiNoch keine Bewertungen
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- Kidney Anatomy PhysiologyDokument26 SeitenKidney Anatomy PhysiologyAlexandra Demian CrisanNoch keine Bewertungen
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- Male Infertility - Understanding, Causes and Treatment PDFDokument497 SeitenMale Infertility - Understanding, Causes and Treatment PDFWaleedNoch keine Bewertungen
- Structures and Functions: Chapter 45: Nursing Assessment: Urinary SystemDokument18 SeitenStructures and Functions: Chapter 45: Nursing Assessment: Urinary SystemKennette LimNoch keine Bewertungen
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (344)
- Urogenital and Reproductive Female. Carangian and SiribanDokument14 SeitenUrogenital and Reproductive Female. Carangian and SiribanKariza AbuNoch keine Bewertungen
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- Acute Scrotal Pain - 2Dokument52 SeitenAcute Scrotal Pain - 2surajit chandNoch keine Bewertungen
- 2 Congenital AbnormalitiesDokument14 Seiten2 Congenital AbnormalitiesSamba SukanyaNoch keine Bewertungen
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- Lesson 1: Identifying and Describing The Parts of The Female Reproductive SystemDokument82 SeitenLesson 1: Identifying and Describing The Parts of The Female Reproductive SystemLendel Mariz O. CepilloNoch keine Bewertungen
- Boala Polichistica Hepato-RenalaDokument1 SeiteBoala Polichistica Hepato-RenaladoinaNoch keine Bewertungen
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- Hypospadias: by Khaled Ashour John Radcliffe HsopitalDokument87 SeitenHypospadias: by Khaled Ashour John Radcliffe Hsopitalhayssam rashwanNoch keine Bewertungen
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- Urinary Pics ADokument22 SeitenUrinary Pics A46bwilsonNoch keine Bewertungen
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2259)
- Hypospadias: Case ReportDokument24 SeitenHypospadias: Case Reportbudi haryadiNoch keine Bewertungen
- Presentation On Urinary CatheterDokument28 SeitenPresentation On Urinary Cathetersushma shresthaNoch keine Bewertungen
- MODULE 15 - Urinary SystemDokument34 SeitenMODULE 15 - Urinary Systemjayc lopezNoch keine Bewertungen
- What Is A CystosDokument4 SeitenWhat Is A CystosStepyn SalvadorNoch keine Bewertungen
- Biology of Human Reproductive SystemDokument51 SeitenBiology of Human Reproductive Systemlen lehangNoch keine Bewertungen
- Chapter 007Dokument7 SeitenChapter 007api-281340024Noch keine Bewertungen
- Reading: Reviewer in Science 5Dokument2 SeitenReading: Reviewer in Science 5Joice Ann PolinarNoch keine Bewertungen
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (120)
- Curriculum Guide: R U A A E CDokument10 SeitenCurriculum Guide: R U A A E CMerce Tojino ManigosNoch keine Bewertungen
- Pex 09 04Dokument4 SeitenPex 09 04DominiqueLovesAmaurionnaSmith33% (9)
- Pressure Flow Urodynamic Studies: The Gold Standard For Diagnosing Bladder Outlet ObstructionDokument8 SeitenPressure Flow Urodynamic Studies: The Gold Standard For Diagnosing Bladder Outlet ObstructionmarcelloNoch keine Bewertungen
- S10 Q3 WEEK1 Reproductive System LECTUREDokument35 SeitenS10 Q3 WEEK1 Reproductive System LECTUREREGLOS, Marie Nhelle K.Noch keine Bewertungen
- UtiDokument41 SeitenUtiKetaks MooNoch keine Bewertungen
- Renal or Urinary Tract DisorderDokument6 SeitenRenal or Urinary Tract DisorderMarcel Quario OrinaNoch keine Bewertungen
- MCQ GenitourinaryDokument3 SeitenMCQ Genitourinaryanojan100% (2)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)