Das könnte Ihnen auch gefallen
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5795)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (345)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (121)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (74)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
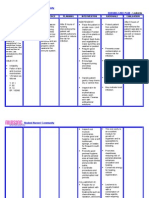
- Nursing Care Plan LeukemiaDokument2 SeitenNursing Care Plan Leukemiaderic87% (30)
- UrticariaDokument21 SeitenUrticariaSumon GhoshNoch keine Bewertungen
- Nts Tevta Test 22-03-15 Paper BDokument2 SeitenNts Tevta Test 22-03-15 Paper BBeTechieNoch keine Bewertungen
- Guidance For Fully Vaccinated PeopleDokument6 SeitenGuidance For Fully Vaccinated PeopleJim Hoft0% (1)
- Giardia LambliaDokument40 SeitenGiardia LambliaKotilakshmanareddy TetaliNoch keine Bewertungen
- Solowska Et Al DX and MGT of COVID Vaccine ReactionsDokument31 SeitenSolowska Et Al DX and MGT of COVID Vaccine ReactionsJoshua TamayoNoch keine Bewertungen
- Non-Gonococcal Urethritis (NGU) : Signs and SymptomsDokument2 SeitenNon-Gonococcal Urethritis (NGU) : Signs and SymptomsIkhfa Yusril BahariNoch keine Bewertungen
- Zhang Et Al-2019-Frontiers in MicrobiologyDokument11 SeitenZhang Et Al-2019-Frontiers in MicrobiologyhadeelNoch keine Bewertungen
- L30 - FPSC Paper Mill Colony C38/1, Gurdwara Road, Siddheshwar LucknowDokument4 SeitenL30 - FPSC Paper Mill Colony C38/1, Gurdwara Road, Siddheshwar LucknowShamsuddin ShamsNoch keine Bewertungen
- Orbital CellulitisDokument21 SeitenOrbital CellulitisElsa Octavia100% (1)
- Primary Health CareDokument54 SeitenPrimary Health CareAretecode777Noch keine Bewertungen
- Preventive MedicineDokument5 SeitenPreventive Medicinescribdnotes123Noch keine Bewertungen
- Henoch - Schonlein Purpura (HSP) : - It Is The Most Common Cause of Non-Thrombocytopenic Purpura in ChildrenDokument23 SeitenHenoch - Schonlein Purpura (HSP) : - It Is The Most Common Cause of Non-Thrombocytopenic Purpura in ChildrenLaith DmourNoch keine Bewertungen
- Neonatal Necrotizing Enterocolitis - Pathology and Pathogenesis - UpToDateDokument21 SeitenNeonatal Necrotizing Enterocolitis - Pathology and Pathogenesis - UpToDateSamuel Idrogo AlfaroNoch keine Bewertungen
- Necrotizing Fasciitis: David Hough MSIII Penn State College of MedicineDokument33 SeitenNecrotizing Fasciitis: David Hough MSIII Penn State College of Medicineaaz220Noch keine Bewertungen
- ImmunisationDokument29 SeitenImmunisationOjambo FlaviaNoch keine Bewertungen
- Antiviral DrugsDokument2 SeitenAntiviral DrugsEzraai HafizNoch keine Bewertungen
- List of Human DiseasesDokument11 SeitenList of Human DiseasesRavi PrakashNoch keine Bewertungen
- PBL Modul 2 TropisDokument31 SeitenPBL Modul 2 TropiskasmaNoch keine Bewertungen
- The 8 Most Common Food AllergiesDokument13 SeitenThe 8 Most Common Food Allergiesfelize padllaNoch keine Bewertungen
- K1. Elektif ParasitDokument34 SeitenK1. Elektif ParasitUu'ayu UnyuNoch keine Bewertungen
- Prevention of RH AlloimmunizationDokument9 SeitenPrevention of RH AlloimmunizationanembrionadoNoch keine Bewertungen
- Balantidium ColiDokument12 SeitenBalantidium Colidaenil_oliverNoch keine Bewertungen
- Reading in B CellsDokument13 SeitenReading in B CellsoaifoiweuNoch keine Bewertungen
- Covid 3Dokument5 SeitenCovid 3api-559328651Noch keine Bewertungen
- Pathophysiology of Meningococcal Meningitis and SepticaemiaDokument8 SeitenPathophysiology of Meningococcal Meningitis and SepticaemiaEugen TarnovschiNoch keine Bewertungen
- Nur81 Drug Study - Metronidazole CefuroximeDokument3 SeitenNur81 Drug Study - Metronidazole CefuroximeJordan GonzalesNoch keine Bewertungen
- Nri1201 Hiv PosterDokument1 SeiteNri1201 Hiv Posteranirbanmanna88320100% (1)
- 1150 3362 1 PBDokument6 Seiten1150 3362 1 PBRoni HasibuanNoch keine Bewertungen
- LA 3 Analytical ExpositionDokument2 SeitenLA 3 Analytical ExpositionVina RohmatikaNoch keine Bewertungen