Das könnte Ihnen auch gefallen
- Original Research Abstract AFCC ASMIHA 2019Dokument82 SeitenOriginal Research Abstract AFCC ASMIHA 2019Program Studi Kardiologi100% (1)
- Drugs Derived From Pigs and Their Clinical AlternativesDokument30 SeitenDrugs Derived From Pigs and Their Clinical Alternativesyeopmi0% (1)
- 4.krisis Hipertensi IMELS 15Dokument41 Seiten4.krisis Hipertensi IMELS 15putusanggraNoch keine Bewertungen
- IMELS New Approach in Basic Life SupportDokument28 SeitenIMELS New Approach in Basic Life SupportAstri Arri FebriantiNoch keine Bewertungen
- Kegawatan Bidang Penyakit Dalam GELSDokument55 SeitenKegawatan Bidang Penyakit Dalam GELSwibowo0% (1)
- 2021 AHA ASA Guideline For The Prevention of Stroke in Patients With Stroke and TIA Clinical UpdateDokument43 Seiten2021 AHA ASA Guideline For The Prevention of Stroke in Patients With Stroke and TIA Clinical Updatejulioel1nico20100% (1)
- PERKENI (2021) - Konsensus DM Tipe 2Dokument119 SeitenPERKENI (2021) - Konsensus DM Tipe 2Ammalia RachmiNoch keine Bewertungen
- MMN Pulmo Full Rezy PDFDokument102 SeitenMMN Pulmo Full Rezy PDFmataNoch keine Bewertungen
- Laporan Kasus KADDokument43 SeitenLaporan Kasus KADharasthaNoch keine Bewertungen
- Bell KJ Thesis 2 PDFDokument84 SeitenBell KJ Thesis 2 PDFlifeinhimNoch keine Bewertungen
- Endocrine DisordersDokument28 SeitenEndocrine DisordersRhitzle Ann50% (2)
- Pro MetricDokument138 SeitenPro Metricahmed100% (8)
- Krisis Hipertensi IMELSDokument43 SeitenKrisis Hipertensi IMELSrinadi_aNoch keine Bewertungen
- Materi 12 IMELS - Trombosis Emboli Paru, Iskemik Tungkai Akut - KritisDokument64 SeitenMateri 12 IMELS - Trombosis Emboli Paru, Iskemik Tungkai Akut - KritismaharyadyNoch keine Bewertungen
- DIC - IMELS (Compatibility Mode)Dokument30 SeitenDIC - IMELS (Compatibility Mode)Astri Arri FebriantiNoch keine Bewertungen
- IPD - Kardiologi PDFDokument114 SeitenIPD - Kardiologi PDFAnnisa Rahmadhania100% (1)
- Lapsus Dr. DodyDokument36 SeitenLapsus Dr. DodyPriscilla Christina NatanNoch keine Bewertungen
- (CKD-MBD) : Chronic Kidney Disease - Mineral and Bone DisorderDokument41 Seiten(CKD-MBD) : Chronic Kidney Disease - Mineral and Bone DisorderronyheryadiNoch keine Bewertungen
- Krisis Tiroid FixDokument38 SeitenKrisis Tiroid FixVita DesriantiNoch keine Bewertungen
- IV Insulin Infusion Protocol TexasDokument2 SeitenIV Insulin Infusion Protocol TexasJohb CaballeroNoch keine Bewertungen
- Morning Report CKDDokument15 SeitenMorning Report CKDMuhammad Haris FirdausNoch keine Bewertungen
- Eimed 2Dokument6 SeitenEimed 2Herik Hamzah0% (4)
- Hipertensi Emergensi (Herbesser)Dokument41 SeitenHipertensi Emergensi (Herbesser)riski novika100% (1)
- Tatalaksana Adiksi NAPZA-Intoksikasi-Adhi Wibowo Nurhidayat-PIT PDUI 2015Dokument97 SeitenTatalaksana Adiksi NAPZA-Intoksikasi-Adhi Wibowo Nurhidayat-PIT PDUI 2015NurcahyaKuswardhanaNoch keine Bewertungen
- CBC GuidelineDokument95 SeitenCBC GuidelineYoung MilkNoch keine Bewertungen
- Physiology CO Guyton ModelDokument42 SeitenPhysiology CO Guyton Modelcovid kojaNoch keine Bewertungen
- A N e M I ADokument21 SeitenA N e M I Anovriadi suhendraNoch keine Bewertungen
- Braunwald Textbook of Cardiovascular Heart Disease 9th - CHM - 00Dokument4 SeitenBraunwald Textbook of Cardiovascular Heart Disease 9th - CHM - 00Teguh RahNoch keine Bewertungen
- BORANGDokument33 SeitenBORANGDewi WangsaNoch keine Bewertungen
- Comprehensive Management SarcopeniaDokument25 SeitenComprehensive Management SarcopeniaMardikaNoch keine Bewertungen
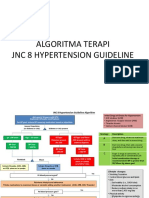
- 2 Algoritma HT JNC 8Dokument3 Seiten2 Algoritma HT JNC 8Nais Maghfiroh100% (1)
- AscitesDokument31 SeitenAscitesHans NatanaelNoch keine Bewertungen
- Konsensus GERD PGI PDFDokument44 SeitenKonsensus GERD PGI PDFMirza ZakaNoch keine Bewertungen
- Adult Vaccination Recommendation: Putu Janu Eka SaputraDokument30 SeitenAdult Vaccination Recommendation: Putu Janu Eka SaputraAndreas HansNoch keine Bewertungen
- JNC 6 Vs 7Dokument2 SeitenJNC 6 Vs 7Diwan AyuNoch keine Bewertungen
- Steps EchoDokument2 SeitenSteps EchoBagus Andi PramonoNoch keine Bewertungen
- Case Krisis HipertensiDokument51 SeitenCase Krisis HipertensianitatiurNoch keine Bewertungen
- Pembahasan UKDI CLINIC 1 Batch Mei 2016Dokument535 SeitenPembahasan UKDI CLINIC 1 Batch Mei 2016William Hartanto RusliNoch keine Bewertungen
- Materi Krisis Tiroid PPDSDokument10 SeitenMateri Krisis Tiroid PPDSRudy Arindra WijayaNoch keine Bewertungen
- Taco and Trali: Savita HandayaniDokument12 SeitenTaco and Trali: Savita HandayaniAnna Puteri GozaliNoch keine Bewertungen
- Sindrom KardiorenalDokument12 SeitenSindrom KardiorenalAndreAHutasoitNoch keine Bewertungen
- PERDICIDokument31 SeitenPERDICIDeya PrastikaNoch keine Bewertungen
- CVP Guided Deresuscitation in Managing Overload in Icu PDFDokument57 SeitenCVP Guided Deresuscitation in Managing Overload in Icu PDFJonathan Hamm100% (1)
- CBT 4 InternaDokument30 SeitenCBT 4 InternaDenny Bimatama100% (3)
- Protap NTG DripDokument4 SeitenProtap NTG DripAinil MardiahNoch keine Bewertungen
- DR. ARIFIN - CAP (New PDPI Guideline)Dokument36 SeitenDR. ARIFIN - CAP (New PDPI Guideline)Inggriht Senny BondangNoch keine Bewertungen
- Journal Reading AminophyllineDokument76 SeitenJournal Reading AminophyllinePandhu Suprobo100% (1)
- 1.2. PneumothoraxDokument42 Seiten1.2. PneumothoraxFarahRullyta100% (1)
- Target Range For Glycemic Control: 80-140 MG/DL (Generally 110 MG/DL)Dokument3 SeitenTarget Range For Glycemic Control: 80-140 MG/DL (Generally 110 MG/DL)Otchi Pudtrie Wijaya100% (1)
- CHF FC III Ec Mitral StenosisDokument36 SeitenCHF FC III Ec Mitral Stenosisbroken18bear100% (1)
- Anti Angina (Hany)Dokument51 SeitenAnti Angina (Hany)Angga AhadiyatNoch keine Bewertungen
- Laporan Kasus: Seorang Laki-Laki Dewasa Dengan CHFDokument33 SeitenLaporan Kasus: Seorang Laki-Laki Dewasa Dengan CHFanizatunNoch keine Bewertungen
- Papdi 2019Dokument1.100 SeitenPapdi 2019Aditya Purwaka100% (3)
- CKDMMM 150717231019 Lva1 App6892 PDFDokument47 SeitenCKDMMM 150717231019 Lva1 App6892 PDFTabada NickyNoch keine Bewertungen
- Hipertensi EmergensiDokument37 SeitenHipertensi EmergensiRisma J AsifNoch keine Bewertungen
- Dr. Risna Weil's DiseaseDokument36 SeitenDr. Risna Weil's DiseasedrroytambunanNoch keine Bewertungen
- Final Cardiovascular Unhas 2013Dokument18 SeitenFinal Cardiovascular Unhas 2013Habi Septiati MusinNoch keine Bewertungen
- Diabetes Mellitus Part 2 - Prof - AskandarDokument40 SeitenDiabetes Mellitus Part 2 - Prof - AskandarAdekresnaHernataNoch keine Bewertungen
- Algorithm For Management of Acute Pulmonary Oedema PDFDokument1 SeiteAlgorithm For Management of Acute Pulmonary Oedema PDFDewi Rabiatul AkhzamiNoch keine Bewertungen
- Kad HHS 2019Dokument35 SeitenKad HHS 2019Friska RamadayantiNoch keine Bewertungen
- Diabetic Ketoacidosis (DKA) : Myocardial InfarctionDokument5 SeitenDiabetic Ketoacidosis (DKA) : Myocardial InfarctionManju PillaiNoch keine Bewertungen
- DKA Protocol With Calculation SheetDokument7 SeitenDKA Protocol With Calculation SheetAmanda Marie Best OsbourneNoch keine Bewertungen
- A K N H: Evidence Based Clinical Practice Guidelines For The Management of Pediatric DKADokument16 SeitenA K N H: Evidence Based Clinical Practice Guidelines For The Management of Pediatric DKAAL AHLINoch keine Bewertungen
- Alert Medical Series: Internal Medicine Alert I, II, IIIVon EverandAlert Medical Series: Internal Medicine Alert I, II, IIINoch keine Bewertungen
- Preoperative Conference Scoliosis Correction-22052926Dokument22 SeitenPreoperative Conference Scoliosis Correction-22052926Demograf27Noch keine Bewertungen
- Regimen TH SimptomatisDokument2 SeitenRegimen TH SimptomatisDemograf27Noch keine Bewertungen
- Instructions For 2019-Ncov Ab Test (Colloidal Gold) : Product Name Intended UseDokument2 SeitenInstructions For 2019-Ncov Ab Test (Colloidal Gold) : Product Name Intended UseDemograf27Noch keine Bewertungen
- Daftar Dosis Dan Sediaan Obat Untuk Anak 160207084634Dokument5 SeitenDaftar Dosis Dan Sediaan Obat Untuk Anak 160207084634Demograf27Noch keine Bewertungen
- Work Resume TemplateDokument2 SeitenWork Resume TemplateDemograf27Noch keine Bewertungen
- Insulin and The Oral HypoglycemicsDokument9 SeitenInsulin and The Oral HypoglycemicsHasibNoch keine Bewertungen
- Carb Counting... Eat To Win!Dokument31 SeitenCarb Counting... Eat To Win!emanvitoriaNoch keine Bewertungen
- Effect of Combined Leaf Extracts of Vernonia (Bitter Leaf) and Gongronema latifolium (Utazi) on the Pancreatic β-Cells of Streptozotocin-Induced Diabetic RatsDokument11 SeitenEffect of Combined Leaf Extracts of Vernonia (Bitter Leaf) and Gongronema latifolium (Utazi) on the Pancreatic β-Cells of Streptozotocin-Induced Diabetic RatsAngga RanggaNoch keine Bewertungen
- Pharm Exam 4 ReviewDokument2 SeitenPharm Exam 4 ReviewHwi GNDCNoch keine Bewertungen
- Pre Gestational ConditionsDokument17 SeitenPre Gestational Conditionslarissedeleon100% (2)
- Basal Bolus InsulinDMT22009Dokument92 SeitenBasal Bolus InsulinDMT22009scribdNoch keine Bewertungen
- Biotechnology: Quarter 2 - Module 4-5 Week 4-5 - Biotechnology and HealthDokument31 SeitenBiotechnology: Quarter 2 - Module 4-5 Week 4-5 - Biotechnology and HealthSheena Mae A. ComingNoch keine Bewertungen
- Insulin, Oral Hypoglycaemic Agents, GlucagonDokument63 SeitenInsulin, Oral Hypoglycaemic Agents, GlucagonBhavesh kunvarNoch keine Bewertungen
- Types of Insulin For Diabetes TreatmentDokument8 SeitenTypes of Insulin For Diabetes TreatmentChander KantaNoch keine Bewertungen
- Handbook of Diabetes Technology 2019 PDFDokument125 SeitenHandbook of Diabetes Technology 2019 PDFPradeep100% (1)
- Pep Mock Exam Questions Updated - 2Dokument84 SeitenPep Mock Exam Questions Updated - 2Cynthia ObiNoch keine Bewertungen
- Akash BhaiyaDokument56 SeitenAkash Bhaiyasai project50% (2)
- MNT - T2DM - 2nd EditionDokument52 SeitenMNT - T2DM - 2nd EditionYi Teng SohNoch keine Bewertungen
- Diabetes Acog 2017Dokument15 SeitenDiabetes Acog 2017Holger Vicente Guerrero Guerrero100% (1)
- Diabetes Pancreatitis: J. Urquiza Z. M.C. F.CDokument42 SeitenDiabetes Pancreatitis: J. Urquiza Z. M.C. F.CgianmarcoNoch keine Bewertungen
- Antidiabetic Drugs: Raymund N. Tapaoan, RPHDokument23 SeitenAntidiabetic Drugs: Raymund N. Tapaoan, RPHNicole EncinaresNoch keine Bewertungen
- JBDS Diabetes at The Front Door Updated September 2021Dokument26 SeitenJBDS Diabetes at The Front Door Updated September 2021jihanNoch keine Bewertungen
- Anti Diabetes MellitusDokument21 SeitenAnti Diabetes MellitusTheresia Merdeka PutriNoch keine Bewertungen
- Diabetic Ketoacidosis and Hyperosmolar Hyperglycemic State in Adults - Treatment - UpToDateDokument36 SeitenDiabetic Ketoacidosis and Hyperosmolar Hyperglycemic State in Adults - Treatment - UpToDateHiKa SaGoNoch keine Bewertungen
- Nur 105 Adult Health I: Diabetes MellitusDokument70 SeitenNur 105 Adult Health I: Diabetes MellitusrikramNoch keine Bewertungen
- Metabolism: 10.1016/j.metabol.2015.12.007Dokument31 SeitenMetabolism: 10.1016/j.metabol.2015.12.007Nurul Kamilah SadliNoch keine Bewertungen
- Top 40 Drugs and Nle FeedbacksDokument106 SeitenTop 40 Drugs and Nle FeedbacksGeraldin Buyagao Kinlijan100% (1)
- Anesthesiology Case PresDokument26 SeitenAnesthesiology Case PresNasrah N. MusaNoch keine Bewertungen
- Canine Diabetes MellitusDokument6 SeitenCanine Diabetes MellitusLauura Cristina BarriosNoch keine Bewertungen
- Quality Assurance For PharmacyDokument6 SeitenQuality Assurance For PharmacyYetiSamaniegoNoch keine Bewertungen
- Ipd - Kelas Ac - Kad Dan Hhs - DR - DR.K Heri Nugroho HS, SP - PD, K-EmdDokument51 SeitenIpd - Kelas Ac - Kad Dan Hhs - DR - DR.K Heri Nugroho HS, SP - PD, K-EmdTeresia MaharaniNoch keine Bewertungen