Das könnte Ihnen auch gefallen
- TetanusDokument32 SeitenTetanusVinotheran MichaelNoch keine Bewertungen
- Chat GPT DAN and Other JailbreaksDokument11 SeitenChat GPT DAN and Other JailbreaksNezaket Sule ErturkNoch keine Bewertungen
- Epidemiology: Aureus and GABHS 10% of The Time. Methicillin-Resistant S Aureus (MRSA) HasDokument8 SeitenEpidemiology: Aureus and GABHS 10% of The Time. Methicillin-Resistant S Aureus (MRSA) HasPutra YdpaNoch keine Bewertungen
- Impetigo: Idowu O. A RN, M.SCDokument15 SeitenImpetigo: Idowu O. A RN, M.SCDebby Love GoodluckNoch keine Bewertungen
- Background: Group A StreptococcusDokument4 SeitenBackground: Group A StreptococcusCoral Srinivasa RamaluNoch keine Bewertungen
- ImpetigoDokument24 SeitenImpetigoIvan Sitohang100% (2)
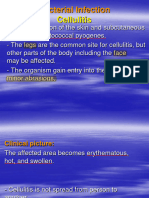
- 3.bacterial Infection-2Dokument146 Seiten3.bacterial Infection-2Biruk WorkuNoch keine Bewertungen
- Impetigo2Dokument4 SeitenImpetigo2Coral Srinivasa RamaluNoch keine Bewertungen
- Bacterial Infections of The Skin, Soft TissuesDokument27 SeitenBacterial Infections of The Skin, Soft TissuesSHIHAB UDDIN KAZI100% (1)
- Communicable Disease Lectures 2Dokument10 SeitenCommunicable Disease Lectures 2NadeshikoNoch keine Bewertungen
- Derma 2Dokument40 SeitenDerma 2tyleree3Noch keine Bewertungen
- Tom Son 2007Dokument7 SeitenTom Son 2007riedha_chanzNoch keine Bewertungen
- Impetigo in Children: A Clinical Guide and Treatment OptionsDokument2 SeitenImpetigo in Children: A Clinical Guide and Treatment OptionsBeuty SavitriNoch keine Bewertungen
- Communicable Disease Lectures 2Dokument2 SeitenCommunicable Disease Lectures 2Sheana TmplNoch keine Bewertungen
- Erbil Polythecnic University Soran Technical Insititute Midwifery Dipartment First Stage (M)Dokument13 SeitenErbil Polythecnic University Soran Technical Insititute Midwifery Dipartment First Stage (M)Kubra ĖdrisNoch keine Bewertungen
- Scabies and ImpetigoDokument13 SeitenScabies and ImpetigoValabhoju Bindu MadhaviNoch keine Bewertungen
- Impetigo Is Caused by Bacteria, Specifically TwoDokument6 SeitenImpetigo Is Caused by Bacteria, Specifically Twoivy2910324Noch keine Bewertungen
- Tinea Cruris Imp Points With ReferencesDokument35 SeitenTinea Cruris Imp Points With ReferencesSyed Saqib AliNoch keine Bewertungen
- Son OdtDokument8 SeitenSon OdtAnonymous sV7PyHXbW5Noch keine Bewertungen
- N11 Chan Chloe Micropara 103 Compilation of Microbial Diseases Final RequirementDokument46 SeitenN11 Chan Chloe Micropara 103 Compilation of Microbial Diseases Final RequirementCHLOE CATHERINE CHANNoch keine Bewertungen
- Chapter 5 Bacterial Diseases of Ruminants 2020Dokument30 SeitenChapter 5 Bacterial Diseases of Ruminants 2020JAD IMADNoch keine Bewertungen
- Diagnosis and Treatment of ImpetigoDokument9 SeitenDiagnosis and Treatment of Impetigonisha_furiNoch keine Bewertungen
- What Is ImpetigoDokument4 SeitenWhat Is ImpetigoKate Mylhen Espenido EnerlanNoch keine Bewertungen
- Bullous Impetigo Is Caused by Staphylococci Producing Exfoliative Toxin That Contains Serine Proteases Acting On Desmoglein 1Dokument2 SeitenBullous Impetigo Is Caused by Staphylococci Producing Exfoliative Toxin That Contains Serine Proteases Acting On Desmoglein 1Justine MayNoch keine Bewertungen
- ImpetigoDokument7 SeitenImpetigoBenjamin VanlaltlansangaNoch keine Bewertungen
- Skin Bacterial Diseases - Part - IDokument9 SeitenSkin Bacterial Diseases - Part - IElijah WoodNoch keine Bewertungen
- ImpetigoDokument13 SeitenImpetigoTasya SyafhiraNoch keine Bewertungen
- Unit 4 BacteriologyDokument51 SeitenUnit 4 BacteriologySharmila LamisharNoch keine Bewertungen
- Skin Diseases PresentationDokument23 SeitenSkin Diseases PresentationDaniTadeNoch keine Bewertungen
- Trachoma Tetanus LeprosyDokument40 SeitenTrachoma Tetanus LeprosyOsama adel Mohamed SmadiNoch keine Bewertungen
- 38 ListerioseDokument4 Seiten38 Listeriosetrs1234Noch keine Bewertungen
- Neonatal InfectionsDokument18 SeitenNeonatal InfectionsSanthosh.S.U100% (1)
- By-Dr. Samarjeet Kaur JR-II BRD Med. College GKPDokument17 SeitenBy-Dr. Samarjeet Kaur JR-II BRD Med. College GKPSamarjeet Kaur100% (1)
- IMPETIGODokument10 SeitenIMPETIGOafifulichwan18Noch keine Bewertungen
- Erbil Polythecnic University Soran Technical Insititute Midwifery Dipartment First Stage (M)Dokument14 SeitenErbil Polythecnic University Soran Technical Insititute Midwifery Dipartment First Stage (M)Kubra ĖdrisNoch keine Bewertungen
- Jurnal EditDokument18 SeitenJurnal EditSabriadi NursalNoch keine Bewertungen
- Neonatal InfectionDokument19 SeitenNeonatal InfectionLekshmi ManuNoch keine Bewertungen
- BacteriologyDokument39 SeitenBacteriologyGrape JuiceNoch keine Bewertungen
- ImpetigoDokument2 SeitenImpetigoAMOS MELINoch keine Bewertungen
- l7 Common Bacterial Infection in DermatologyDokument35 Seitenl7 Common Bacterial Infection in DermatologyOmar HamwiNoch keine Bewertungen
- IZZ - PiodermaDokument51 SeitenIZZ - PiodermavivilmNoch keine Bewertungen
- Jurnal Reading KulitDokument26 SeitenJurnal Reading KulitKeyko SeptiyantiNoch keine Bewertungen
- Herpes Simplex Oral: EpidemiologyDokument5 SeitenHerpes Simplex Oral: EpidemiologyFariz RamadhanNoch keine Bewertungen
- Infection & Specific Wound InfectionsDokument39 SeitenInfection & Specific Wound InfectionsAhmed ShorshNoch keine Bewertungen
- Impetigo - Review : Luciana Baptista Pereira1Dokument7 SeitenImpetigo - Review : Luciana Baptista Pereira1Edwar RevnoNoch keine Bewertungen
- Impetigo: By: Keerthi.V Roll - No.59Dokument9 SeitenImpetigo: By: Keerthi.V Roll - No.59Harshal ChavanNoch keine Bewertungen
- Tubkut Srilanka JournalDokument7 SeitenTubkut Srilanka JournalMusdalifah MimousNoch keine Bewertungen
- Disorders of Skin in ChildrenDokument47 SeitenDisorders of Skin in Childrensmriti boraNoch keine Bewertungen
- (ANDREWS) Impetigo, Ecthyma PDFDokument4 Seiten(ANDREWS) Impetigo, Ecthyma PDFmpsoletaNoch keine Bewertungen
- Vesiculobullous DiseasesDokument40 SeitenVesiculobullous Diseasessgoeldoc_550661200100% (1)
- Superficial Skin Infections and The Use of Topical and Systemic Antibiotics in General PracticeDokument4 SeitenSuperficial Skin Infections and The Use of Topical and Systemic Antibiotics in General Practicepeter_mrNoch keine Bewertungen
- (Impetigo) : Erbil Polythecnic University Soran Technical Insititute Nuraing Department First StageDokument14 Seiten(Impetigo) : Erbil Polythecnic University Soran Technical Insititute Nuraing Department First StageKubra ĖdrisNoch keine Bewertungen
- Impetigo: Signs and SymptomsDokument3 SeitenImpetigo: Signs and Symptomspragna novaNoch keine Bewertungen
- Approach To Fever With RashDokument35 SeitenApproach To Fever With RashSenthilnathan ANoch keine Bewertungen
- Bacterial InfectiosnDokument4 SeitenBacterial InfectiosnPatrick Z. MascareñasNoch keine Bewertungen
- Name: Carlo M. Yao Bachelor of Science in NursingDokument33 SeitenName: Carlo M. Yao Bachelor of Science in Nursingcarlo24_briggsNoch keine Bewertungen
- Blistering DisordersDokument7 SeitenBlistering DisordersSaman SarKoNoch keine Bewertungen
- Microbial Diseases of The Different Organ System SKINDokument102 SeitenMicrobial Diseases of The Different Organ System SKINBea Bianca CruzNoch keine Bewertungen
- Artikan 3Dokument1 SeiteArtikan 3Rivan San JayaNoch keine Bewertungen
- ImpetigoDokument8 SeitenImpetigoEmilia Manurun Tangke AlloNoch keine Bewertungen
- Impetigo, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsVon EverandImpetigo, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsBewertung: 5 von 5 Sternen5/5 (3)
- Hermeneutical Phenomenology and Human Enviroment SystemDokument12 SeitenHermeneutical Phenomenology and Human Enviroment SystemAllen Rose Buenaflor BuenoNoch keine Bewertungen
- Allusions and References - 5Dokument3 SeitenAllusions and References - 5Matthew HallingNoch keine Bewertungen
- Parathyroid Agents PDFDokument32 SeitenParathyroid Agents PDFRhodee Kristine DoñaNoch keine Bewertungen
- K Unit 1 SeptemberDokument2 SeitenK Unit 1 Septemberapi-169447826Noch keine Bewertungen
- Detailed Lesson Plan in Tle Grade 8Dokument7 SeitenDetailed Lesson Plan in Tle Grade 8Hanna MikangcrzNoch keine Bewertungen
- Grammar Exercises AnswersDokument81 SeitenGrammar Exercises Answerspole star107100% (1)
- Philippine Literature During American PeriodDokument5 SeitenPhilippine Literature During American PeriodMi-cha ParkNoch keine Bewertungen
- If He Asked YouDokument10 SeitenIf He Asked YouLourdes MartinsNoch keine Bewertungen
- 2 - The British Legal SystemDokument4 Seiten2 - The British Legal SystemSTAN GABRIELA ELENANoch keine Bewertungen
- Swimming Pool - PWTAG CodeofPractice1.13v5 - 000Dokument58 SeitenSwimming Pool - PWTAG CodeofPractice1.13v5 - 000Vin BdsNoch keine Bewertungen
- Logical Remarks On The Semantic Approach PDFDokument34 SeitenLogical Remarks On The Semantic Approach PDFFelipe SantosNoch keine Bewertungen
- SjshagavDokument6 SeitenSjshagavindah ayu lestariNoch keine Bewertungen
- Computerized Dynamic Posturography (CDP)Dokument2 SeitenComputerized Dynamic Posturography (CDP)eldescribdNoch keine Bewertungen
- 1820 Celestial EventDokument8 Seiten1820 Celestial EventDoor Of ElNoch keine Bewertungen
- Pro Angular JS (Apress)Dokument1 SeitePro Angular JS (Apress)Dreamtech PressNoch keine Bewertungen
- 2 Islm WBDokument6 Seiten2 Islm WBALDIRSNoch keine Bewertungen
- F A T City Workshop NotesDokument3 SeitenF A T City Workshop Notesapi-295119035Noch keine Bewertungen
- Battle of The ChoirDokument3 SeitenBattle of The Choirkoizume_reiNoch keine Bewertungen
- Gamma Ray Interaction With Matter: A) Primary InteractionsDokument10 SeitenGamma Ray Interaction With Matter: A) Primary InteractionsDr-naser MahmoudNoch keine Bewertungen
- Apcr MCR 3Dokument13 SeitenApcr MCR 3metteoroNoch keine Bewertungen
- Cayman Islands National Youth Policy September 2000Dokument111 SeitenCayman Islands National Youth Policy September 2000Kyler GreenwayNoch keine Bewertungen
- Rizal Course ReviewerDokument6 SeitenRizal Course ReviewerMarianne AtienzaNoch keine Bewertungen
- Geoland InProcessingCenterDokument50 SeitenGeoland InProcessingCenterjrtnNoch keine Bewertungen
- Minimum Structural Properties and Test Procedure For TG20 Compliant Prefabricated Structural Transom UnitsDokument16 SeitenMinimum Structural Properties and Test Procedure For TG20 Compliant Prefabricated Structural Transom UnitsPrimelift Safety Resources LimitedNoch keine Bewertungen
- Review of Related LiteratureDokument5 SeitenReview of Related LiteratureRJ PareniaNoch keine Bewertungen
- The American New CriticsDokument5 SeitenThe American New CriticsSattigul KharakozhaNoch keine Bewertungen
- Ansys Flu - BatDokument30 SeitenAnsys Flu - BatNikola BoskovicNoch keine Bewertungen
- Ebook PDF The Irony of Democracy An Uncommon Introduction To American Politics 17th Edition PDFDokument42 SeitenEbook PDF The Irony of Democracy An Uncommon Introduction To American Politics 17th Edition PDFscott.stokley449100% (39)
- I. Title: "REPAINTING: Streetlight Caution Signs"Dokument5 SeitenI. Title: "REPAINTING: Streetlight Caution Signs"Ziegfred AlmonteNoch keine Bewertungen