Das könnte Ihnen auch gefallen
- Fast Facts: Deficiencia de piruvato quinasa para pacientes y familiares: Una enfermedad genética rara que afecta a los glóbulos rojos Información + Asumir el control = El mejor resultadoVon EverandFast Facts: Deficiencia de piruvato quinasa para pacientes y familiares: Una enfermedad genética rara que afecta a los glóbulos rojos Información + Asumir el control = El mejor resultadoNoch keine Bewertungen
- Psychosine: Biochemistry '' Biochemistry '' Section IiDokument1 SeitePsychosine: Biochemistry '' Biochemistry '' Section IiMuhammad AbubakarNoch keine Bewertungen
- Fast Facts: Le déficit en pyruvate kinase pour les patients et les accompagnants: Une maladie génétique rare qui affecte les globules rouges Informations + Prise de contrôle = Meilleur résultatVon EverandFast Facts: Le déficit en pyruvate kinase pour les patients et les accompagnants: Une maladie génétique rare qui affecte les globules rouges Informations + Prise de contrôle = Meilleur résultatNoch keine Bewertungen
- Pediatrics Storage DiseasesDokument2 SeitenPediatrics Storage DiseasesuyesNoch keine Bewertungen
- SL - No Diseases Enzyme Defect Lipid Accumulating Salient FeaturesDokument1 SeiteSL - No Diseases Enzyme Defect Lipid Accumulating Salient FeaturesReeba KuruvillaNoch keine Bewertungen
- Diabetes Mellitus 1Dokument5 SeitenDiabetes Mellitus 1smurplerNoch keine Bewertungen
- WWW - Natures.Ir: More Free Usmle, Mccee, Mcqe and Amq FlashcardsDokument54 SeitenWWW - Natures.Ir: More Free Usmle, Mccee, Mcqe and Amq FlashcardsNixon GoyalNoch keine Bewertungen
- Glycogen Storage DiseasesDokument7 SeitenGlycogen Storage DiseasesNikhilBhattNoch keine Bewertungen
- DX: Risiko Infeksi DX: Perubahan Nutrisi Kurang: KematianDokument2 SeitenDX: Risiko Infeksi DX: Perubahan Nutrisi Kurang: KematianLilipory GestiNoch keine Bewertungen
- Storage DisordersDokument1 SeiteStorage DisordersDian Putri NingsihNoch keine Bewertungen
- Enzyme Deficiencies of Glycolysis and TCA: D N D S /SDokument8 SeitenEnzyme Deficiencies of Glycolysis and TCA: D N D S /SJordan WhiteNoch keine Bewertungen
- Biochem Quick Review by Haji MuhammadDokument7 SeitenBiochem Quick Review by Haji Muhammadimran dilawarNoch keine Bewertungen
- B. Pathophysiology A) Schematic Diagram (Book - Based) : Wasting Blood Glucose LevelDokument2 SeitenB. Pathophysiology A) Schematic Diagram (Book - Based) : Wasting Blood Glucose LevelCarl Elexer Cuyugan Ano50% (2)
- Adrenal Control Within The Body: Presented byDokument20 SeitenAdrenal Control Within The Body: Presented byhumnaNoch keine Bewertungen
- Hemolytic Anemia: G6PD Deficiency For The USMLE Step One ExamDokument27 SeitenHemolytic Anemia: G6PD Deficiency For The USMLE Step One ExamJoeNoch keine Bewertungen
- Glycogen, Muco, Lysosomal Storage DseDokument3 SeitenGlycogen, Muco, Lysosomal Storage DseMark Angelo PonferradoNoch keine Bewertungen
- Pathogenesis Chronic Complications DiabetesDokument5 SeitenPathogenesis Chronic Complications DiabetesGerardLum100% (1)
- Carbohydrate Metabolism DisordersDokument14 SeitenCarbohydrate Metabolism DisordersAki OtaniNoch keine Bewertungen
- Sphingolipidosis: Disease Enzyme Deficient Accumulated Product Sings & SymptomsDokument1 SeiteSphingolipidosis: Disease Enzyme Deficient Accumulated Product Sings & Symptomsnreena aslamNoch keine Bewertungen
- Pathology of DiabetesDokument4 SeitenPathology of DiabetesGerardLum100% (4)
- CBS Lipids and Membrane Structure CASE BASED DISCUSSION 22 - 23Dokument11 SeitenCBS Lipids and Membrane Structure CASE BASED DISCUSSION 22 - 23Arm UdomratNoch keine Bewertungen
- PLT DisordersDokument3 SeitenPLT DisordersAudreySlitNoch keine Bewertungen
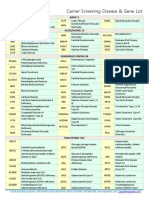
- Carrier Screening Disease & Gene List: Basic 5Dokument3 SeitenCarrier Screening Disease & Gene List: Basic 5Alexandra Ançã Pires100% (1)
- Hypoparathyroidism: A Clinical Casebook Natalie E. CusanoDokument15 SeitenHypoparathyroidism: A Clinical Casebook Natalie E. CusanoOleOhhNoch keine Bewertungen
- HematologyDokument171 SeitenHematologyDanielle FosterNoch keine Bewertungen
- Malarial RXDokument2 SeitenMalarial RXalrainsNoch keine Bewertungen
- Uk CDGDokument4 SeitenUk CDGIon CimirinschiNoch keine Bewertungen
- Thyroid Gland Agenesis/dysgenesisDokument4 SeitenThyroid Gland Agenesis/dysgenesisSerious LeoNoch keine Bewertungen
- Emd166 Slide Acute Coronary PDFDokument40 SeitenEmd166 Slide Acute Coronary PDFlorinsyacderminnatNoch keine Bewertungen
- Kematian: Krsakan Glomerulus SCR ProgresifDokument2 SeitenKematian: Krsakan Glomerulus SCR ProgresifAnnis Laella MegassariNoch keine Bewertungen
- Disease Compendium UpdatedDokument9 SeitenDisease Compendium UpdatedKing-son LinNoch keine Bewertungen
- CR EndokrinDokument14 SeitenCR EndokrinFajar SutrisnaNoch keine Bewertungen
- PharmaDokument6 SeitenPharmanotespreparer11Noch keine Bewertungen
- Gene Related DiseaseDokument3 SeitenGene Related Diseasevivek govardhanamNoch keine Bewertungen
- Swift River Medication AdministrationDokument4 SeitenSwift River Medication AdministrationmattNoch keine Bewertungen
- Stimulate Renin Release: Decreased Blood Flow To O2 KidneyDokument2 SeitenStimulate Renin Release: Decreased Blood Flow To O2 KidneyMiguelito Galagar GultianoNoch keine Bewertungen
- Gangguan Kel. AdrenalDokument16 SeitenGangguan Kel. AdrenalInna Nur Fitri DahliyantiNoch keine Bewertungen
- Marfan Syndrome: Disorder Gene Protein/Abnormal Chrom. Comment/classic FindingsDokument71 SeitenMarfan Syndrome: Disorder Gene Protein/Abnormal Chrom. Comment/classic FindingsAndres TabaresNoch keine Bewertungen
- Diuretics: Na/K/Cl Co-Transporter (NKCC2)Dokument3 SeitenDiuretics: Na/K/Cl Co-Transporter (NKCC2)Safiya JamesNoch keine Bewertungen
- ProstaglandinsDokument29 SeitenProstaglandinsNarasimha MurthyNoch keine Bewertungen
- Pediatrics NephrologyDokument25 SeitenPediatrics NephrologyNujhat TabassumNoch keine Bewertungen
- SBRC General PrinciplesDokument51 SeitenSBRC General Principlesdalia khamoNoch keine Bewertungen
- Diabetes Mellitus: DiagnosisDokument8 SeitenDiabetes Mellitus: DiagnosisKelly YeowNoch keine Bewertungen
- Cardiac GlycosidesDokument10 SeitenCardiac GlycosidesGlupiaSprawaNoch keine Bewertungen
- Some Common Types of Mutation in DnaDokument2 SeitenSome Common Types of Mutation in DnaFer Pineda MinaNoch keine Bewertungen
- 13 08045 Askandar 0840Dokument9 Seiten13 08045 Askandar 0840Fadhil Muhammad AwaluddinNoch keine Bewertungen
- Medical Concept Mapping Type 2 DiabetesDokument1 SeiteMedical Concept Mapping Type 2 DiabetesRENEROSE TORRESNoch keine Bewertungen
- Clin Kidney J 2012 de Baaij I15 24Dokument10 SeitenClin Kidney J 2012 de Baaij I15 24rizki octavianaNoch keine Bewertungen
- Biochemistry: Diseases / Disorders Genetic DisordersDokument3 SeitenBiochemistry: Diseases / Disorders Genetic DisordersKailash KhatriNoch keine Bewertungen
- EhDokument3 SeitenEhYusril MarhaenNoch keine Bewertungen
- Section XIX - Lysosomal Storage Diseases: Disease Deficient Enzyme Accumulated Substrate Findings InheritanceDokument2 SeitenSection XIX - Lysosomal Storage Diseases: Disease Deficient Enzyme Accumulated Substrate Findings InheritanceKatharine NervaNoch keine Bewertungen
- Biochem DiseasesDokument25 SeitenBiochem DiseasesSSGFL1100% (1)
- HemoglobinopathiesDokument3 SeitenHemoglobinopathiesChatie PipitNoch keine Bewertungen
- Liddle, Gitelman, BarterDokument2 SeitenLiddle, Gitelman, BarterHildemaro GutierrezNoch keine Bewertungen
- Screening For Micro and Macrovascular ComplicationDokument38 SeitenScreening For Micro and Macrovascular ComplicationRoby KieranNoch keine Bewertungen
- O High Fat, High Carbohydrate o Caffeinated and Carbonated o 73 Years Old o MaleDokument4 SeitenO High Fat, High Carbohydrate o Caffeinated and Carbonated o 73 Years Old o MaleJoherNoch keine Bewertungen
- Notes: Adrenal HypofunctionDokument4 SeitenNotes: Adrenal HypofunctionWiyosa RusdiNoch keine Bewertungen
- Journal Reading Neurology - Slide 2Dokument10 SeitenJournal Reading Neurology - Slide 2Putri Rahmadhani Ngakpaniklage AsdsNoch keine Bewertungen
- Bleeding Disorders 1 - DR - Kamal MokbelDokument13 SeitenBleeding Disorders 1 - DR - Kamal MokbelRawan E. SaeedNoch keine Bewertungen
- Step 3 - PharmacologyDokument10 SeitenStep 3 - PharmacologyLauren LevyNoch keine Bewertungen
- Dr. Ahaghotu - Urology Physical ExaminationDokument62 SeitenDr. Ahaghotu - Urology Physical Examination13un391543100% (2)
- Endocrine PT IIDokument23 SeitenEndocrine PT II13un391543Noch keine Bewertungen
- Eldra W Daniels Final Write UpDokument3 SeitenEldra W Daniels Final Write Up13un391543Noch keine Bewertungen
- Endocrinology IDokument45 SeitenEndocrinology I13un391543Noch keine Bewertungen
- Step 1 USMLE NotesDokument15 SeitenStep 1 USMLE Notes13un391543100% (1)
- HeadacheDokument20 SeitenHeadache13un391543Noch keine Bewertungen
- Abdominal MassDokument17 SeitenAbdominal Mass13un391543Noch keine Bewertungen
- CoughDokument20 SeitenCough13un391543Noch keine Bewertungen
- Notes For Women in PsychologyDokument23 SeitenNotes For Women in PsychologyAdam PilarskiNoch keine Bewertungen
- Module 3 Gender and SocietyDokument21 SeitenModule 3 Gender and Societyabegail arponNoch keine Bewertungen
- Hormones FTMDokument16 SeitenHormones FTMapi-221867127Noch keine Bewertungen
- Fausto - SterlingDokument35 SeitenFausto - SterlingAlex BlencoweNoch keine Bewertungen
- Obstetric-Gynecology MCQsDokument297 SeitenObstetric-Gynecology MCQsDr Ishtiaq Ahmad88% (125)
- PDFDokument657 SeitenPDFJesús Enrique Turín Vilca100% (1)
- 10 - Vaginal Agenesis - A Systematic ReviewDokument41 Seiten10 - Vaginal Agenesis - A Systematic ReviewNunuh SulaemanNoch keine Bewertungen
- Govind AmbiGen PosterDokument1 SeiteGovind AmbiGen PosterYolanda MNoch keine Bewertungen
- Memorial FinalDokument27 SeitenMemorial Finalp samhithNoch keine Bewertungen
- Scally - Anabolic Steroids - A Question of Muscle PDFDokument253 SeitenScally - Anabolic Steroids - A Question of Muscle PDFpavel100% (1)
- Evaluation and Management of Primary Amenorrhea - UpToDateDokument15 SeitenEvaluation and Management of Primary Amenorrhea - UpToDateGaby GarridoNoch keine Bewertungen
- Approach To A Case of Ambiguous GenitaliaDokument37 SeitenApproach To A Case of Ambiguous GenitaliaDR.MAULIK SHAHNoch keine Bewertungen
- Androgen Insensitivity Syndrome (Ais)Dokument18 SeitenAndrogen Insensitivity Syndrome (Ais)Junbek nov23Noch keine Bewertungen
- Androgen Insensitivity Syndrome: Genetics Home ReferenceDokument5 SeitenAndrogen Insensitivity Syndrome: Genetics Home Referencelaura benavidesNoch keine Bewertungen
- Articles About IntersexualityDokument69 SeitenArticles About IntersexualityRuben MicleaNoch keine Bewertungen
- Me My Sex and I Reflection PaperDokument2 SeitenMe My Sex and I Reflection PaperMeow YoongiNoch keine Bewertungen
- Vaginal AgenesisDokument3 SeitenVaginal Agenesissanks06Noch keine Bewertungen
- Developmental Biology, 12th Edition (Michael J.F. Barresi, Scott F. Gilbert)Dokument48 SeitenDevelopmental Biology, 12th Edition (Michael J.F. Barresi, Scott F. Gilbert)Nita DelinaNoch keine Bewertungen
- Desordenes Del Desarrollo Sexual Copia 2Dokument16 SeitenDesordenes Del Desarrollo Sexual Copia 2mariakjaimesNoch keine Bewertungen
- Morgan Holmes (Ed.) - Critical Intersex PDFDokument274 SeitenMorgan Holmes (Ed.) - Critical Intersex PDFAlbertoReina100% (2)
- Nbme Step 1 AnatomyDokument23 SeitenNbme Step 1 AnatomyMohsin Farooq100% (12)
- Ambiguous GenitaliaDokument24 SeitenAmbiguous GenitaliaYolanda SamsudinNoch keine Bewertungen
- Anatomia y FisiologiaDokument43 SeitenAnatomia y FisiologiaRiky Sanz100% (1)
- Management of The Infant With Atypical Genitalia (Disorder of Sex Development) - UpToDateDokument31 SeitenManagement of The Infant With Atypical Genitalia (Disorder of Sex Development) - UpToDateNicolle SchioNoch keine Bewertungen
- Ambiguous GenitaliaDokument11 SeitenAmbiguous GenitaliadragondostNoch keine Bewertungen
- Dian Ais EditDokument41 SeitenDian Ais EditDian SiregarNoch keine Bewertungen
- 18 Male Hypogonadism LR1Dokument24 Seiten18 Male Hypogonadism LR1Retma Rosela NurkayantyNoch keine Bewertungen
- IntersexnnDokument66 SeitenIntersexnnSyahputraWibowoNoch keine Bewertungen
- Appiah, The Lies That BindDokument16 SeitenAppiah, The Lies That BindMaria Paula Suarez100% (1)
- Sex Chromosomes and Sex DeterminationDokument60 SeitenSex Chromosomes and Sex Determinationstevensb055100% (4)
- The Obesity Code: Unlocking the Secrets of Weight LossVon EverandThe Obesity Code: Unlocking the Secrets of Weight LossBewertung: 4 von 5 Sternen4/5 (5)
- By the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsVon EverandBy the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsNoch keine Bewertungen
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeVon EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeBewertung: 2 von 5 Sternen2/5 (1)
- The Age of Magical Overthinking: Notes on Modern IrrationalityVon EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityBewertung: 4 von 5 Sternen4/5 (24)
- The Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaVon EverandThe Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- Summary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisVon EverandSummary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisBewertung: 4.5 von 5 Sternen4.5/5 (42)
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedVon EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedBewertung: 5 von 5 Sternen5/5 (80)
- ADHD is Awesome: A Guide to (Mostly) Thriving with ADHDVon EverandADHD is Awesome: A Guide to (Mostly) Thriving with ADHDBewertung: 5 von 5 Sternen5/5 (1)
- Self-Care for Autistic People: 100+ Ways to Recharge, De-Stress, and Unmask!Von EverandSelf-Care for Autistic People: 100+ Ways to Recharge, De-Stress, and Unmask!Bewertung: 5 von 5 Sternen5/5 (1)
- Raising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsVon EverandRaising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsBewertung: 5 von 5 Sternen5/5 (1)
- Outlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisVon EverandOutlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisBewertung: 4 von 5 Sternen4/5 (1)
- The Comfort of Crows: A Backyard YearVon EverandThe Comfort of Crows: A Backyard YearBewertung: 4.5 von 5 Sternen4.5/5 (23)
- Dark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Von EverandDark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Bewertung: 4.5 von 5 Sternen4.5/5 (110)
- Gut: the new and revised Sunday Times bestsellerVon EverandGut: the new and revised Sunday Times bestsellerBewertung: 4 von 5 Sternen4/5 (392)
- Why We Die: The New Science of Aging and the Quest for ImmortalityVon EverandWhy We Die: The New Science of Aging and the Quest for ImmortalityBewertung: 4 von 5 Sternen4/5 (3)
- Raising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsVon EverandRaising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsBewertung: 4.5 von 5 Sternen4.5/5 (169)
- Cult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryVon EverandCult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryBewertung: 4 von 5 Sternen4/5 (44)
- Mindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessVon EverandMindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessBewertung: 4.5 von 5 Sternen4.5/5 (328)
- The Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsVon EverandThe Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsBewertung: 3.5 von 5 Sternen3.5/5 (3)
- When the Body Says No by Gabor Maté: Key Takeaways, Summary & AnalysisVon EverandWhen the Body Says No by Gabor Maté: Key Takeaways, Summary & AnalysisBewertung: 3.5 von 5 Sternen3.5/5 (2)
- Sleep Stories for Adults: Overcome Insomnia and Find a Peaceful AwakeningVon EverandSleep Stories for Adults: Overcome Insomnia and Find a Peaceful AwakeningBewertung: 4 von 5 Sternen4/5 (3)
- Gut: The Inside Story of Our Body's Most Underrated Organ (Revised Edition)Von EverandGut: The Inside Story of Our Body's Most Underrated Organ (Revised Edition)Bewertung: 4 von 5 Sternen4/5 (378)
- To Explain the World: The Discovery of Modern ScienceVon EverandTo Explain the World: The Discovery of Modern ScienceBewertung: 3.5 von 5 Sternen3.5/5 (51)
- The Marshmallow Test: Mastering Self-ControlVon EverandThe Marshmallow Test: Mastering Self-ControlBewertung: 4.5 von 5 Sternen4.5/5 (58)