Das könnte Ihnen auch gefallen
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- A) Importance of The Case StudyDokument73 SeitenA) Importance of The Case StudyRaidis PangilinanNoch keine Bewertungen
- Gun BanDokument2 SeitenGun BanNyj QuiñoNoch keine Bewertungen
- GORDONsDokument6 SeitenGORDONsNyj QuiñoNoch keine Bewertungen
- 545Dokument1 Seite545Nyj QuiñoNoch keine Bewertungen
- Intro and Drug StudyDokument14 SeitenIntro and Drug StudyNyj QuiñoNoch keine Bewertungen
- Lesson FlowDokument2 SeitenLesson FlowNyj QuiñoNoch keine Bewertungen
- AntibioticsDokument2 SeitenAntibioticsNyj QuiñoNoch keine Bewertungen
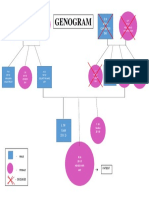
- Genogram ArfDokument1 SeiteGenogram ArfNyj QuiñoNoch keine Bewertungen
- A) Importance of The Case StudyDokument73 SeitenA) Importance of The Case StudyRaidis PangilinanNoch keine Bewertungen
- Case Study On Chronic Kidney Disease Probably To Secondary HypertensionDokument18 SeitenCase Study On Chronic Kidney Disease Probably To Secondary Hypertensionkyeria77% (26)
- Genogram ArfDokument1 SeiteGenogram ArfNyj QuiñoNoch keine Bewertungen
- Curriculum VitaeDokument4 SeitenCurriculum VitaeNyj QuiñoNoch keine Bewertungen
- Case StudyDokument54 SeitenCase StudyNyj QuiñoNoch keine Bewertungen
- Assessment of Home and EnvironmentDokument2 SeitenAssessment of Home and EnvironmentNyj QuiñoNoch keine Bewertungen
- Nursing Updates BlankDokument2 SeitenNursing Updates BlankNyj QuiñoNoch keine Bewertungen
- Case Study NowDokument49 SeitenCase Study NowNyj QuiñoNoch keine Bewertungen
- Case Study NowDokument49 SeitenCase Study NowNyj QuiñoNoch keine Bewertungen
- Zeny 1Dokument2 SeitenZeny 1Nyj QuiñoNoch keine Bewertungen
- Zeny 1Dokument2 SeitenZeny 1Nyj QuiñoNoch keine Bewertungen
- Journal Format - BlankDokument1 SeiteJournal Format - BlankNyj QuiñoNoch keine Bewertungen
- Health TeachingDokument3 SeitenHealth TeachingNyj QuiñoNoch keine Bewertungen
- FNCPDokument3 SeitenFNCPNyj QuiñoNoch keine Bewertungen
- Nursing Updates BlankDokument2 SeitenNursing Updates BlankNyj QuiñoNoch keine Bewertungen
- Journal Format - BlankDokument1 SeiteJournal Format - BlankNyj QuiñoNoch keine Bewertungen
- Adherence To Therapies Is A Primary Determinant of Treatment SuccessDokument7 SeitenAdherence To Therapies Is A Primary Determinant of Treatment SuccessNyj QuiñoNoch keine Bewertungen
- Managing Your Blood Sugar PDFDokument2 SeitenManaging Your Blood Sugar PDFNyj QuiñoNoch keine Bewertungen
- Ovarian 20 Cancer 1Dokument39 SeitenOvarian 20 Cancer 1Muhammad AL Farisi SutrisnoNoch keine Bewertungen
- Syllabus On Alternative Pain Management Techniques: Foundation UniversityDokument25 SeitenSyllabus On Alternative Pain Management Techniques: Foundation UniversityNyj QuiñoNoch keine Bewertungen
- Coursematerial 136Dokument13 SeitenCoursematerial 136Nyj QuiñoNoch keine Bewertungen
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (344)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (399)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (73)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2259)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (120)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- DysrhythmiasDokument67 SeitenDysrhythmiashhh hhhNoch keine Bewertungen
- Final Pharmacokinetics Workshop (Consized) - 1Dokument17 SeitenFinal Pharmacokinetics Workshop (Consized) - 1Adlina TajuddinNoch keine Bewertungen
- APPENDIX A B GlossaryDokument15 SeitenAPPENDIX A B GlossaryaddiramonaNoch keine Bewertungen
- COAP Forum CollectionDokument6 SeitenCOAP Forum Collectionprashmanic100% (1)
- NEET PG Previous Year Questions 2021Dokument144 SeitenNEET PG Previous Year Questions 2021medpoxNoch keine Bewertungen
- Drugs For Congestive Heart FailureDokument46 SeitenDrugs For Congestive Heart Failuresultan khabeeb100% (1)
- Cardiac DrugsDokument107 SeitenCardiac DrugscomgmailNoch keine Bewertungen
- Nursing Management of Patient With CCFDokument34 SeitenNursing Management of Patient With CCFJayarani Ashok100% (1)
- Verapamil PDFDokument13 SeitenVerapamil PDFddandan_2Noch keine Bewertungen
- USNI Medication TestDokument8 SeitenUSNI Medication Testusni100% (31)
- NCLEX Review NotesDokument20 SeitenNCLEX Review Notesshaali86Noch keine Bewertungen
- Pharmacology ReviewerDokument21 SeitenPharmacology ReviewerCzairalene QuinzonNoch keine Bewertungen
- Cardiovascular Drugs - Nurse - DR DianDokument67 SeitenCardiovascular Drugs - Nurse - DR DianAndyk Strapilococus Aureus100% (2)
- Rationale-Heart FailureDokument17 SeitenRationale-Heart FailureRI NANoch keine Bewertungen
- Drug Study - DigoxinDokument2 SeitenDrug Study - DigoxinKian Herrera50% (2)
- Practice Dosage ExamDokument6 SeitenPractice Dosage Examstarshine70006Noch keine Bewertungen
- 004 LabsDiagnosticsManualDokument64 Seiten004 LabsDiagnosticsManualRaju Niraula100% (1)
- Essential Notes in Internal Medicine - 1st EdDokument163 SeitenEssential Notes in Internal Medicine - 1st EdEhsanullah HikmatNoch keine Bewertungen
- PNLE III Nursing PracticeDokument11 SeitenPNLE III Nursing PracticeASDF ASDFNoch keine Bewertungen
- Planned Parenthood Sues To Block Ohio Ban On Dilation and Evacuation AbortionDokument16 SeitenPlanned Parenthood Sues To Block Ohio Ban On Dilation and Evacuation AbortionWCPO 9 NewsNoch keine Bewertungen
- Assignment Repeat MacrogolDokument40 SeitenAssignment Repeat MacrogolAnthony HartNoch keine Bewertungen
- Drug Formulary HospitalDokument98 SeitenDrug Formulary HospitalahmshmNoch keine Bewertungen
- Digoxi N: Therapeutic Drug Monitoring ofDokument17 SeitenDigoxi N: Therapeutic Drug Monitoring ofsky.blueNoch keine Bewertungen
- Study Guide For Pharmacology and The Nursing Process e Book 8th Edition Ebook PDFDokument53 SeitenStudy Guide For Pharmacology and The Nursing Process e Book 8th Edition Ebook PDFalfred.jessie484100% (40)
- Heart Failure: Zelalem T., MD Yr III Resident, PediatricsDokument65 SeitenHeart Failure: Zelalem T., MD Yr III Resident, PediatricsChalie MequanentNoch keine Bewertungen
- BretyliumDokument4 SeitenBretyliumButchay LumbabNoch keine Bewertungen
- 2.20140209 Question PaperDokument16 Seiten2.20140209 Question PaperdrpnnreddyNoch keine Bewertungen
- DRUG StudyDokument18 SeitenDRUG StudyMargaux Moir0% (1)
- Toxicology Lecture 5 - DigoxinDokument29 SeitenToxicology Lecture 5 - DigoxinyousernameNoch keine Bewertungen
- Pharm Drugs ListDokument14 SeitenPharm Drugs ListHumbe Oshun100% (1)